
There are many, many people out there who question whether lockdowns, masks and other ‘restrictions’ are actually more damaging to people’s health, mental health and the economy than the disease itself. This often leads them to conclude that we shouldn’t have lockdowns and that we should somehow simply ‘protect the vulnerable’ and let everyone else continue life as normal.
There are many parts to unpick with this concept. It is totally understandable that people may want to ask the question, but it is really important that the answers come from a place of reliable data and evidence rather than emotive claims.
So, I’m going to have a go at looking at some of the issues regularly raised by so-called ‘lockdown sceptics’ and their supporters and what the available evidence actually shows.
“Why enforce masks when they’ve been proven not to work?”
Masks have not been ‘proven not to work’. A review of over 140 studies and academic papers found overwhelming evidence to support the wearing of masks to prevent the spread of Covid-19. It found:
- If at least 70 per cent of people wore masks, modelling suggests that combined with contact tracing, that would be sufficient to stop the epidemic growing.
- People are most infectious before developing symptoms making widespread mask use, whether you have symptoms or not, absolutely vital.
- All types of material are helpful at preventing the spread of the disease from an infected carrier, although some are better than others.
- Masks offer some protection to the wearer, although the primary benefit is in preventing infectious people from spreading the virus.
They also found an American economic analysis suggesting universal mask wearing could add 1 trillion dollars to the US GDP.
“Masks do more harm than good.”

There have been suggestions that mask wearing would lead to people getting complacent about other measures such as distancing and handwashing. Similar arguments about risk behaviour were made about motorbike helmets, seatbelts, and ski helmets when they were introduced and were equally unfounded. Observational data during the pandemic has shown that mask wearers are better at hand hygiene, distancing and reduced face touching. There is also data to suggest that mask wearing acts as a cue to others to keep their distance.
There has also been a suggestion that masks can cause bacterial pneumonia, but this is simply not true. There appear to be no records showing it happening anywhere, despite the claim, and doctors have explained that the only thing that ends up on your face mask is what you breath out. For your exhaled breath to contain pneumonia-causing bacteria it would have to be in your lungs already.
“I know someone who always wore a mask and they still caught Covid-19, so they obviously don’t work.”
The primary benefit of mask wearing is to protect those around you. There has been shown to be some protective effect on the wearer, but not as strong as the effect they have on protecting those around you.
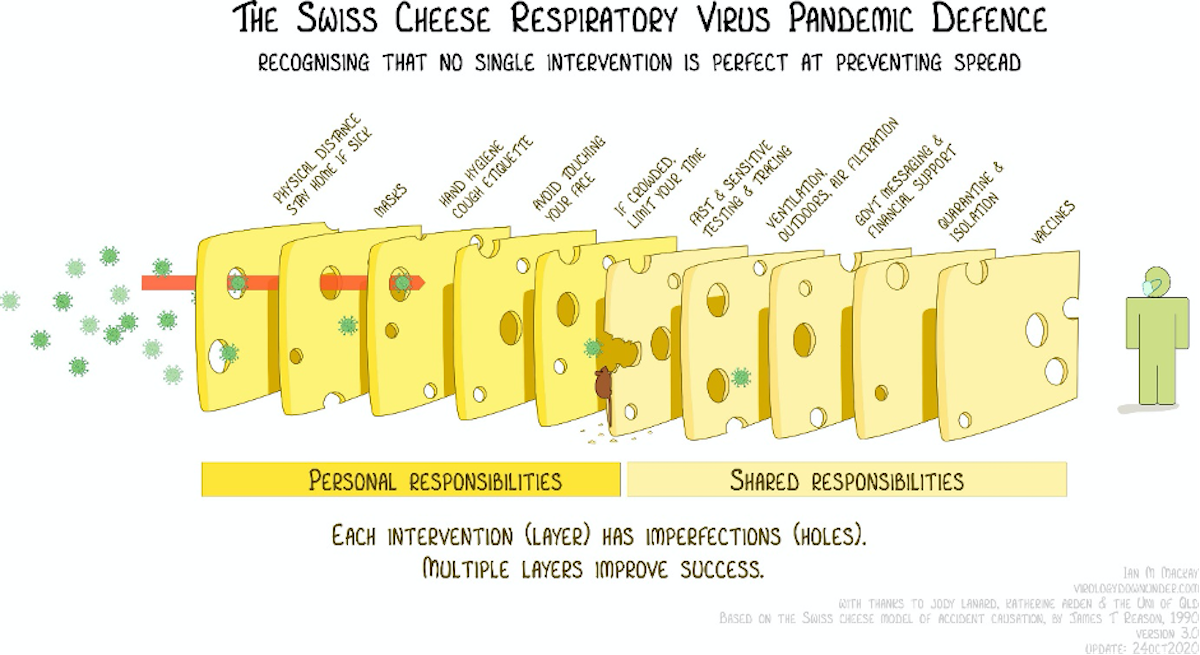
No measure will be 100 per cent effective in stopping the pandemic, but multiple measures used together are our best shot.
“Lockdowns don’t work.”
Covid-19 can only spread by people mixing. It cannot spread without a human involved. So just on a purely logical level, staying at home as much as possible will prevent the virus from spreading.
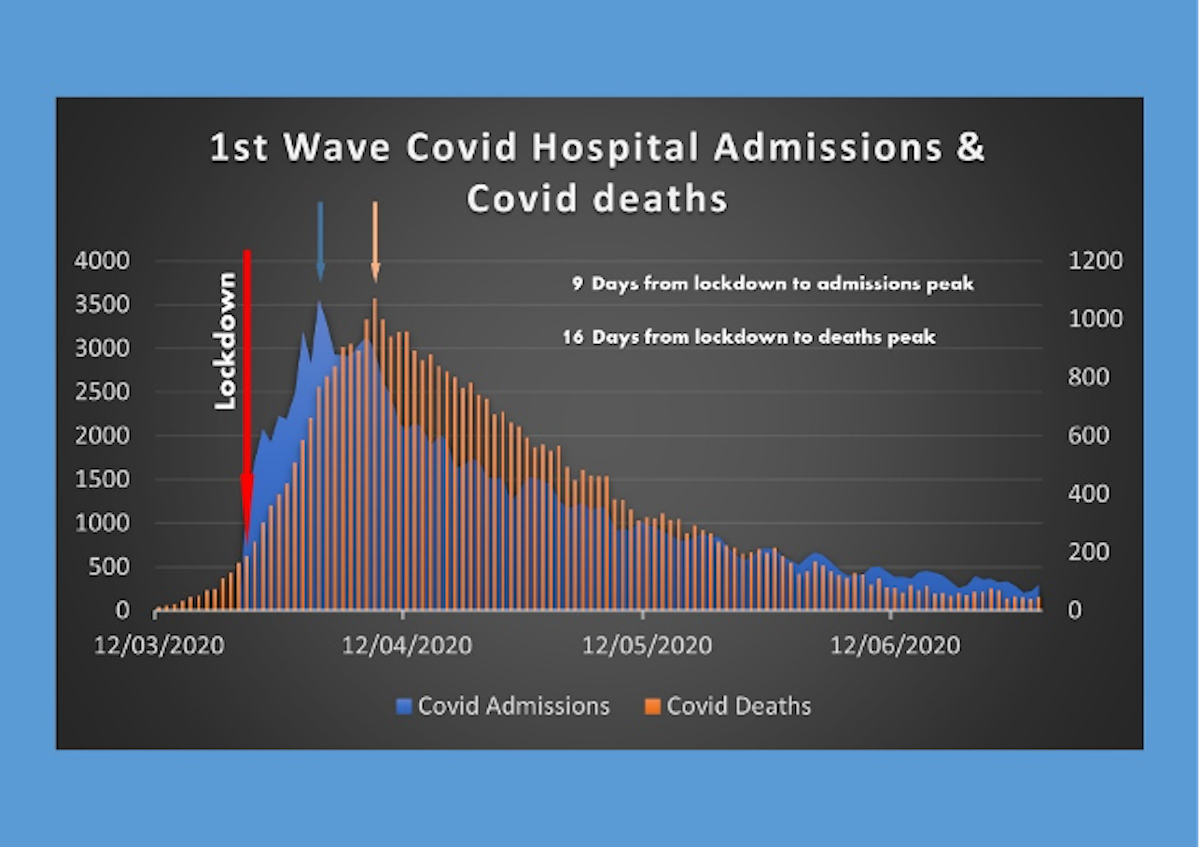
There is a time lag between restrictions being put in place and the effects being seen in either hospital admissions or deaths recorded. It takes up to 14 days for symptoms to appear (average length five days after infection), an average of 3-10 days between symptoms and hospital admissions, and an average of two weeks between symptoms and death.
Looking at the first lockdown in the spring, you can see that hospital admissions started falling after around 9 days, while deaths started falling about a week later. This is entirely in line with the timings you would expect to see if it were the lockdown restrictions that were limiting cases.
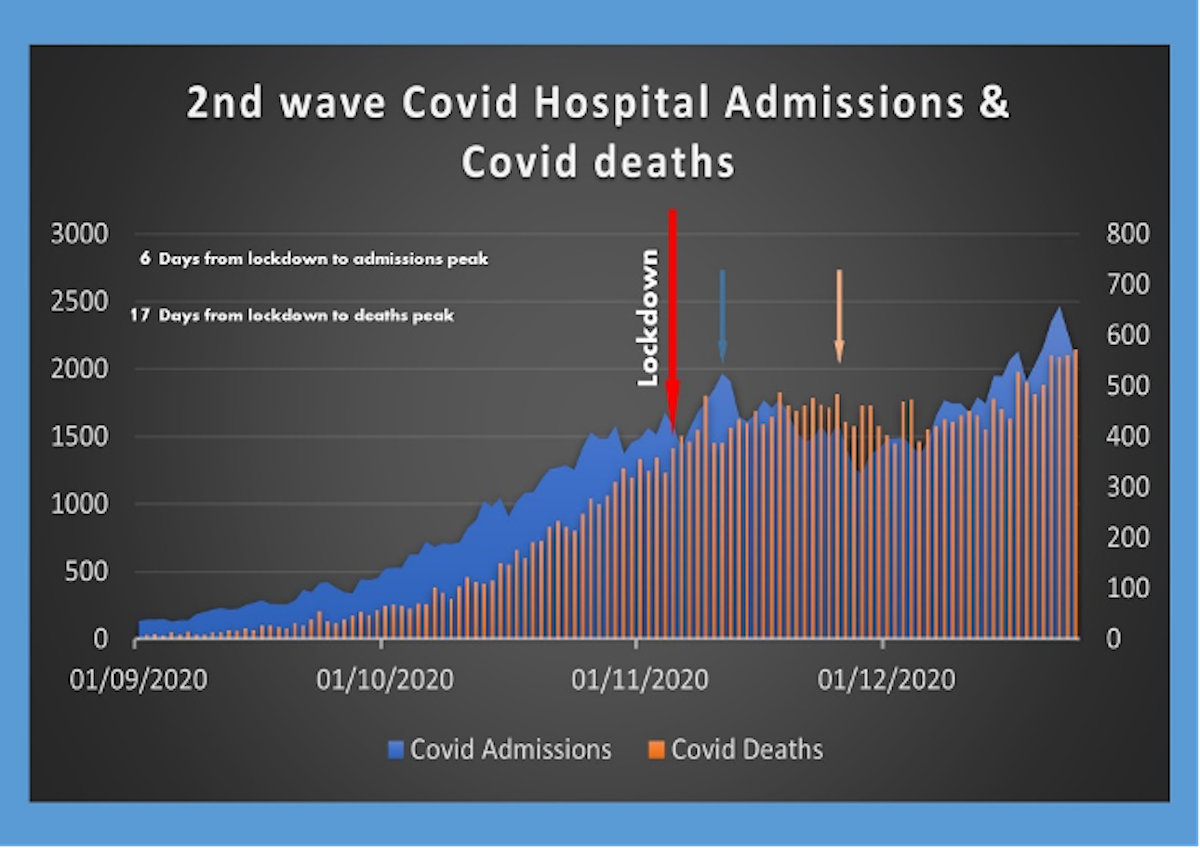
The second lockdown in November was much looser, so did not have the same dramatic effect that the first lockdown did. The time lags were still indicative of the restrictions having a significant effect on slowing the spread of Covid-19. Unfortunately, the effects were quickly wiped out by shopping and mixing in the run up to Christmas.
“Lockdowns have completely trashed the economy.”
Lockdowns do have a major effect on the economy, as retail, manufacturing, hospitality, live events etc., all have to stop.
However, it is not as straightforward as that. Had there not been a lockdown, retail, hospitality and live events would still have been hit hard by people choosing to stay at home for fear of catching the virus, and by people being unable to work through sickness, and sadly, death.
One of the arguments put forward to delaying lockdown back in spring was to ‘keep the economy going as long as possible’, but unfortunately this argument didn’t play out well.
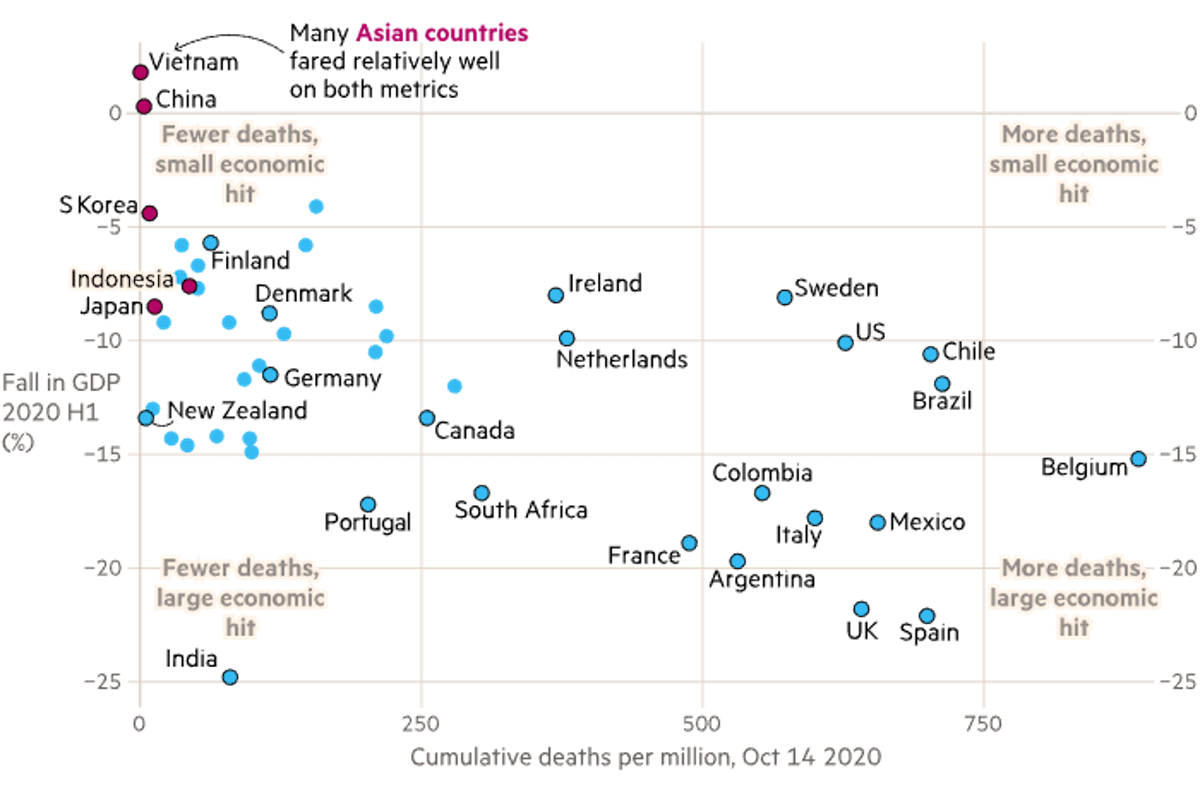
Analysis has shown that the countries that got the spread of the virus under control the most effectively, often by locking down hard and fast, ended up with a far lesser impact on their economy. The UK was one of the worst performing in both the economy and number of deaths, as shown in this graph from Covid-19: The global crisis — in data.
The argument that you have to balance health with wealth is a false dichotomy. A healthy population is intrinsically linked to a healthy economy and you cannot have one without the other.
“Scientists forcing lockdowns on us predicted there would be 500,000 deaths in the UK, but they were wrong – we never should have locked down based on their data.”
Neil Ferguson published a modelling report in March that showed if we took no steps at all to curb the spread of the virus, we could see 550,000 deaths over 2 years as a result. The point of the modelling was to decide which steps would be most effective in suppressing the virus and saving lives. Many steps were then taken to limit the spread, including social distancing, encouraging handwashing, closing mass gatherings, closing schools and other lockdown measures. All these interventions played a role in slowing the spread of the virus, limiting the number of people who became infected and therefore the number of people who died.
The fact that 550,000 people did not die does NOT mean those steps were not needed. It shows the opposite.
“But what about Sweden? They didn’t lockdown and they were ok.”
Sweden chose a quite different route to dealing with the pandemic and was hailed as a success by many lockdown sceptics early on. They chose to ban large gatherings, close their airports, move high schools and universities to distance learning, and encourage working from home, but kept junior schools, non-essential shops, bars, and restaurants open, albeit with social distancing guidelines in place.
Unfortunately, Sweden ended up with one of the highest per capita death tolls in the world AND took a greater financial hit than other similar economies.
Authorities in Sweden have been widely criticized, with some apologising for failing to protect the elderly and nursing home residents.
“Lockdowns have stopped us from being able to develop herd immunity.”
Some people were calling for a ‘herd immunity’ strategy from early on. The UK and Sweden appear to have been the only countries planning to follow that path.
The idea was to protect the vulnerable and allow the virus to spread through the rest of the population, allowing them to build up immunity. If enough people have immunity, the population is said to have ‘herd immunity’ – where people are protected by the fact that others are immune, and the disease won’t spread.
However, there has never been a human virus that has reached a high enough level of herd immunity to protect the vulnerable, without a vaccine. Even if it were possible, it would require at least 70 per cent of the population to have been infected and developed immunity. As this virus has a mortality rate of one per cent, it would lead to around 500,000 people dying in the UK alone. The evidence on whether you end up with long term immunity from contracting the disease is also not clear.
Sweden hoped that their light touch lockdown would have at least increased their levels of immunity, however widespread studies of antibody levels have shown that only 17 per cent of residents in Stockholm had immunity by the summer, with levels of only four per cent elsewhere in Sweden. London also showed around 17 per cent with five per cent elsewhere in England.
{kind=link}
“Lockdowns have huge impact on mental health.”
Most people are justifiably concerned about the effects of lockdown on the mental health of the population. The ONS (Office for National Statistics) routinely survey people to get a snapshot of how the nation is feeling. It is clear that people are feeling less happy, less satisfied with life and more anxious than they were in February 2020. What is less clear is whether this change is as a result of the lockdowns themselves or a result of the pandemic in general. For example, anxiety levels were at their highest in March, improving during the summer. However, the lockdown in November did not appear to impact the levels at all. They have gone up again at the start of January, but whether that is down the worsening news regarding new variants, overcrowded hospitals or the prospect of the lockdown, is hard to tell.

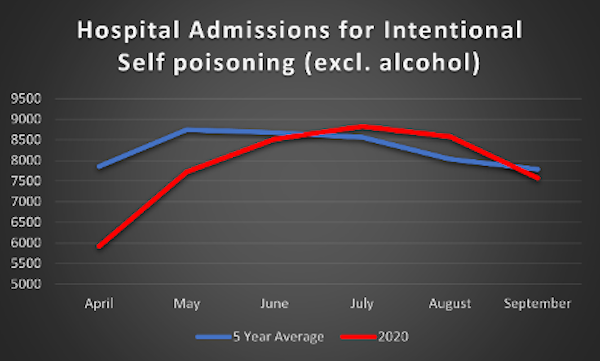
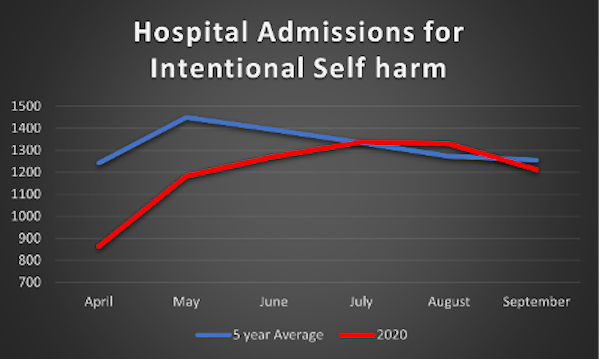
“Lockdowns have caused a massive increase in self-harm and suicides.”
There have been concerns regarding the levels of self-harm and suicides that could be caused by lockdowns, with many mental health organisations warning of severe impacts on mental health from loneliness, isolation and money concerns. However, it is hard to quantify these effects. Data shown here looks at the number of hospital admissions for self-harm and self-poisoning each month between April and September 2020 compared to the average for each month in the last 5 years. April, May and June (during lockdown) all saw lower than average numbers, with numbers being slightly higher than average during the summer months. This does not support the theory that lockdowns caused an increase in self harming.
A Study by Manchester University looked at suicide figures from established ‘real-time surveillance’ systems in several parts of England, comparing the months pre-lockdown (January-March 2020) to post-lockdown (April-August 2020). The average number of suicides per month varied but there was no evidence of a rise post-lockdown. They caveated the report by saying that the study only covered parts of England (population of around nine million), and they could not rule out a future rise as the economic impact of the pandemic continues to take its toll.
A British Medical Journal editorial examined the available data from across the world relating to suicide rates during lockdown and concluded “Nevertheless, a reasonably consistent picture is beginning to emerge from high income countries. Reports suggest either no rise in suicide rates (Massachusetts, USA; Victoria, Australia; England) or a fall (Japan, Norway) in the early months of the pandemic. The picture is much less clear in low- income countries, where the safety nets available in better resourced settings may be lacking.”
There is absolutely no question people are suffering as a result of the lockdowns. But it is really important to also understand that without the lockdowns, the suffering may have been just as much of a problem as many more people would have lost loved ones, and the economy would likely have been equally badly hit (see section above on economy).
“Lockdown meant hospitals stopped treating anyone else. They were only interested in Covid-19 Patients.”
This is a common misconception. The hospitals did not ‘close’ during lockdown. They continued to treat anyone who needed emergency treatment, as long as they had the staff and ICU (Intensive Care Unit) capacity. Non-emergency, routine surgery needed to be cancelled as staff were deployed to other areas of the hospital. Surgery always comes with a risk of requiring intensive care, so cancelling these types of surgeries ensured the ICUs were available for critical patients.
Once a hospital reaches capacity, whether with Covid-19 patients, flu patients, or stroke and heart attacks, then the ability to treat anyone disappears, regardless of the need. So, an ICU full of Covid-19 patients means there is no room for the car crash victim or meningitis case. This is why the primary reason given for lockdowns is to prevent the hospitals becoming overrun with Covid-19 patients. Keeping numbers down is the best way to save lives from any cause – not just from Covid-19.
Dr Pimenta illustrates it nicely:
It is worth noting that in countries which dealt swiftly and successfully with their Covid-19 outbreaks, access to healthcare for other reasons was not impacted on the scale we have seen in the UK. In May, the World Health Organisation (WHO) sent a survey to 194 ministries of Health, of whom 163 responded. The results showed that less than 50 per cent of countries saw disruption to their cancer services, emergency dental care, diabetes care, asthma services or palliative care. In the UK, the fifth richest nation and the second most pandemic prepared country (on paper!) we saw widespread disruption to our health services. This is more a reflection of our poor response and long-term poor funding of our health service, than a direct consequence of lockdown.
“Lockdown caused more deaths than Covid-19.”
Some headlines have claimed that the lockdown itself was going to cause ‘more deaths than covid-19’. However, there does not appear to be any factual basis to these claims – other than the opinion of the journalists!
Many papers ran with the headline in July that an ONS report had estimated that lockdown would result in an additional 200,000 deaths. However, when looking at the report itself, this is only half the story. It estimates the number of deaths due to delayed healthcare, suicides, domestic abuse, people being scared to go to hospital etc., following a lockdown. These were around 200,000 in the long term, in addition to the 45,000 predicted Covid-19 deaths at the time. Then, the report compared this to the number of deaths estimated if no lockdown had been implemented. These were estimated at 450,000 Covid-19 deaths and more than 1,000,000 deaths as a direct result of people not being able to access hospital care due to over-run hospitals.
So, although the effects of reduced hospital care during lockdown could lead to significant lives lost in the future, NOT locking down would likely have led to around five times that number in non-Covid-19 deaths, and double that number in Covid-19 deaths.
“Can’t we just protect the vulnerable and let everyone else live life as normal, like they suggested with the Great Barrington Declaration?”
The Great Barrington Declaration was written by 3 scientists and funded by right wing climate change denier Charles Koch and supposedly signed up to by 8000 scientists. However, many of these have been proven to be fake signatories, including Dr Sciency McScienceface and Dr Wibbleton Wibbler! Anyone could sign it with no authentication or confirmation of their credentials needed. It has been widely discredited by the scientific and medical communities.
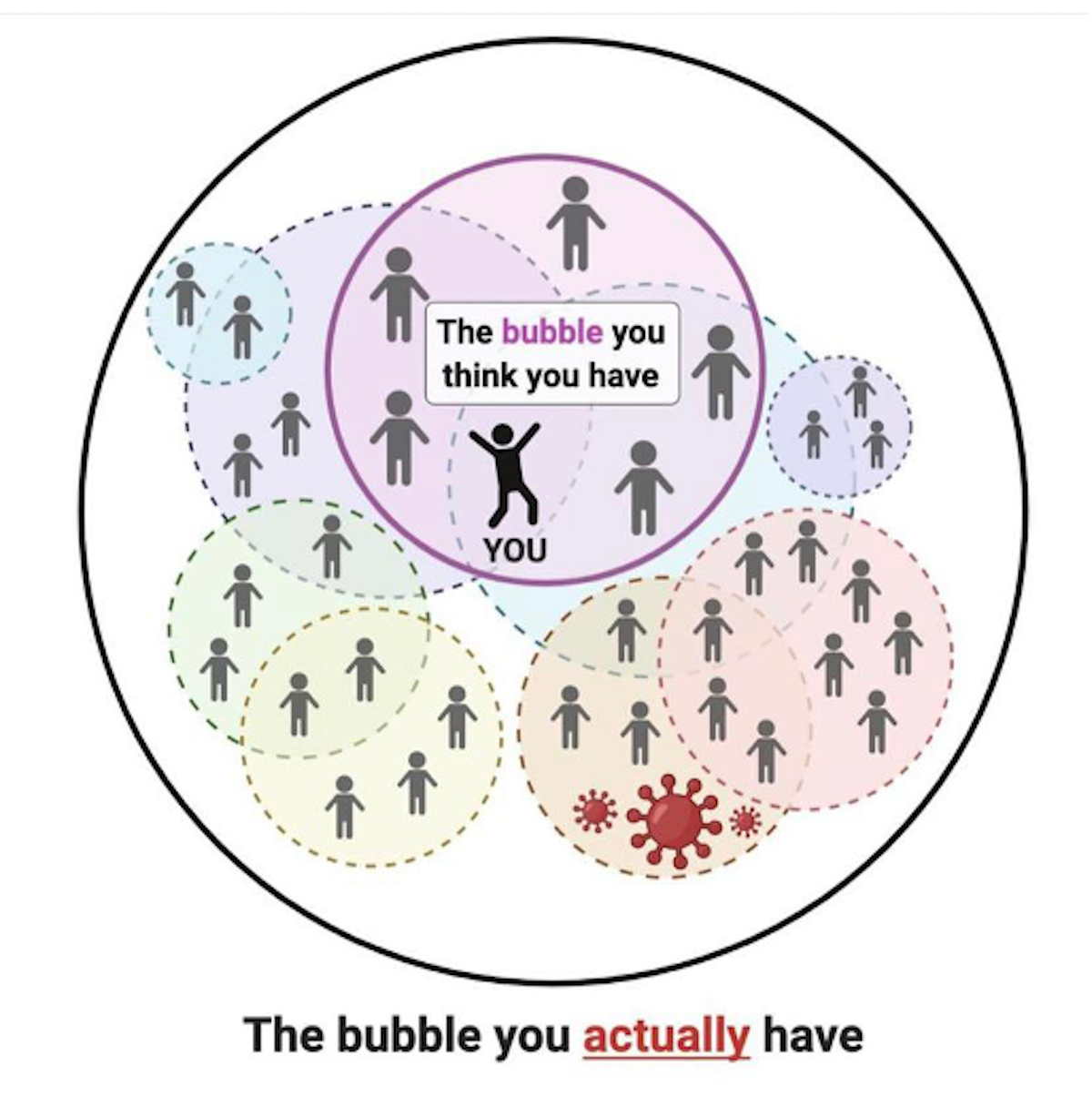
The idea was a vague notion that you could somehow lock away the ‘vulnerable’ while allowing everyone else to carry on as normal. There were no suggestions on how this would actually work in principle. Our lives are highly interconnected, as illustrated below, with every visit to buy food, collect medicine or receive care leading to the vulnerable coming into contact with those ‘carrying on as normal’.
There are just over 10 million people in the UK in the extremely high risk categories (over 70s and Extremely Clinically Vulnerable), with a further 17.2 million considered moderately high risk (50-70 year olds and those with underlying conditions that put them ‘at risk’ from Covid-19). The idea that 14-40 per cent of the UK population could be kept completely shielded from the rest of the population is just simply unworkable. Not to mention the massive hit the economy would take from the working aged vulnerable people being unable to work, or any of the vulnerable being unable to go to garden ientres, shops, restaurants etc.
It is also worth mentioning that although the risk of death from Covid-19 in the younger age groups is low, there is a lot of evidence coming out now of long-term health risks, known as ‘Long-Covid’, associated with even mild cases of the disease. The long-term effects on the healthcare system and the economy are likely to be significant, and the more you allow the virus to spread, the more people are likely to end up in this category.
In addition, the more people you allow to contract Covid-19 the higher the chances of new, more transmissible (catching) strains of Covid-19 developing, as we have seen with the new B117 variant.
Conclusion
Keeping the virus numbers under control requires multiple restrictions, including mask wearing and social distancing. In an ideal world (as has been seen in many other countries) large scale testing, rapid and efficient track and trace systems, and enforced quarantining would keep numbers low enough to allow life to return to normal and protect lives. Unfortunately, in the absence of those measures, lockdowns are the only way to stop the virus killing hundreds of thousands of people.
No one denies that lockdowns come with a hefty price, both on mental health and the economy, but so does an uncontrolled pandemic. Imagine your house was on fire, but a sprinkler system managed to put out the flames. You might rightly complain that now all your belongings were wet, but that is infinitely preferable to them being destroyed by the fire. So it is with lockdowns. The consequences are problematic, but the consequence of not having them is far, far worse.




