One of the areas where I keep coming across a lot of misinformation relates to testing ‒polymerase chain reaction (PCR), lateral flow tests (LFT), false positives, false negatives, and whether the inventor of PCR really said PCR shouldn’t be used to test for Covid-19!
It is easy to get confused by the different molecular biology techniques when you see information being reported in news articles and on social media, so I will try, as always, to cover as many topics as I can and make it as simple as I can!
First, I’ll briefly cover the three main methods used when testing for Covid-19:
- PCR (specifically rt-PCR)
PCR is a molecular biology technique used to amplify DNA in a sample, enough times for it to be detectable in a lab. The coronavirus that causes Covid-19 is called SARS-CoV-2. This virus is made from RNA (a slightly different form of genetic material), so it needs to be converted into DNA at the start of the process using an enzyme called reverse transcriptase (that’s the ‘rt’ bit in rt-PCR). Watch here for a short video explaining rt-PCR testing for Covid-19.
PCR is used to determine if someone is currently infected with the virus. It is an incredibly accurate technique but needs specialist equipment and can take up to a couple of days to get a result back.
- Lateral Flow Tests (LFT)
Lateral flow tests are a type of antigen test, similar to a pregnancy test, which are used to detect a piece of the virus itself, usually a bit of protein from the outside of the virus. Watch here for a short video explaining how these tests work.
LFTs are also used to determine if someone is currently infected with the virus. They are not as good at giving a positive result as PCR is, so a negative LFT result is not a reliable way of proving you do not have Covid-19. However, they are quick and cheap, and provide a useful mass testing method in schools or workplaces.
- Antibody Tests
Antibody tests are blood tests used to check whether you have antibodies to the SARS-CoV-2 virus. Watch here for a short video explaining how these tests work.
Antibody tests are used to determine whether you have antibodies to the Covid-19 virus and were therefore exposed to the virus previously. It cannot give you information on whether you are currently infected with Covid-19.
So now you have a little more information on what the tests are and how they work, I will dive right into some of the misinformation making its way round the internet.
“The PCR tests detect any virus so a positive result means you might just have a cold.”
PCR is a very specific technique, which involves amplifying DNA many, many times until there is enough present to be seen using particular lab techniques. The beauty of PCR is that the parts of the test that are required for amplification to work ‒ called primers ‒ only stick to the DNA if their genetic code completely matches the genetic code of the virus. Scientists have used the exact genetic code to work out which sections of RNA are unique to SARS-CoV-2 and have designed these primers to stick only to that code. No other virus exists with those short sequences and so no other virus can be detected using this PCR test.
PCR tests exist for lots of other viruses, each completely specific to the virus it is designed to detect. The SARS-CoV-2 PCR test was used on samples known to contain all sorts of other viruses including adenovirus, several influenza types, multiple parainfluenzas, human bocavirus, rhinovirus/enterovirus, and many more. All the results came back negative. This shows that the Covid-19 PCR test does not give a positive result unless SARS-CoV-2 is present, regardless of what other viruses may be there.
“Most of the so-called ‘cases’ are false positives.”
This is simply untrue. The false positive rate (FPR) of PCR is incredibly low. Unfortunately, a misunderstanding of the statistics around the specificity and sensitivity of PCR by key figures in the media, alongside MPs such as Dominic Raab, led to a widespread belief that false positives were a big problem. Figures ranging from one per cent to 93 per cent false positive rates were all over social media back in the summer.
There are a number of pieces of evidence showing that false positive rates are incredibly low and that case numbers in the UK are not due to false positives:
- Since the start of the pandemic, New Zealand has run 1.75m tests and has found 2,389 cases. Even if every single one of them was a false positive (which they weren’t!) that would give an FPR of only 0.14 per cent.
- The Office for National Statistics (ONS) calculated the false positive rate in the UK is less than 0.005 per cent.
- In the summer in the UK, when Covid-19 levels were at their lowest, 150,000 tests per day were being performed but were only finding several hundred cases. If they were all false positives, that would be a FPR of 0.2 per cent. We know that these were not all false positives, as people were still dying and being treated for Covid-19 infections in hospital.
- The same PCR test protocol is performed all around the world. If false positives really were an issue, it would be hard to explain why some countries such as New Zealand and Singapore got incredibly low numbers, while countries such as the UK and Belgium were getting high ones. The fact that different countries have different results shows that there is not an inherent problem with the test itself.
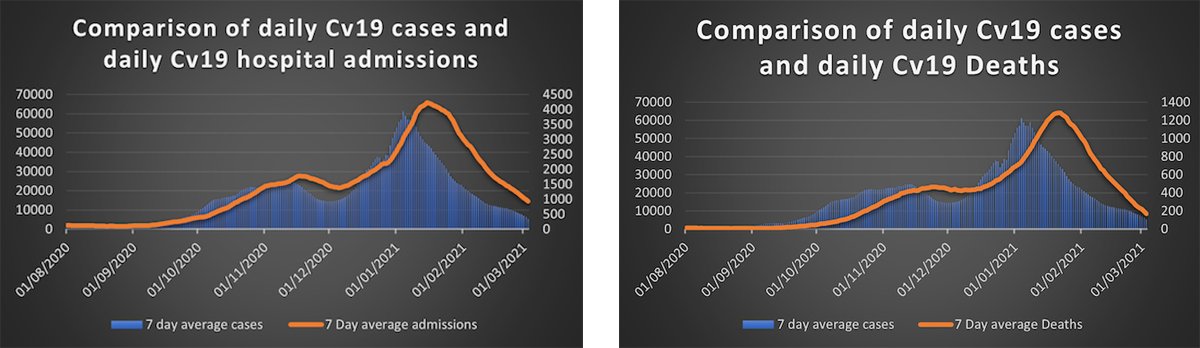
- The final and most obvious piece of evidence we have is that case numbers rise and fall in line with both Covid-19 hospital admissions and Covid-19 deaths.
The take-home message is that PCR is incredibly sensitive. It will only produce a positive result if there is SARS-CoV-2 genetic material present. All the furore around false positives was simply a distraction used by lockdown opponents, who don’t understand PCR, to try and discredit case numbers.
It’s also worth noting that PCR using nasal swabs is far more likely to produce a false negative result than a false positive one. Depending on which day of infection the swab is taken, the chance of getting a false negative PCR test due to too little detectable virus, ranges from 20 per cent to 100 per cent. In the same way that taking a pregnancy test too early will give you a negative result, so can Covid-19 tests taken too early in an infection. This has a far greater effect on the case numbers than the miniscule proportion that may be false positives.
“We only have more cases in the UK than other countries because we test more people.”
It is certainly true that if countries don’t do very much testing, they will be reporting far fewer Covid-19 cases, as a result of the lack of testing. But there is a fairly simple method for looking to see whether a country is testing enough to give an accurate picture.
The test positivity rate (TPR) of a country looks at how many tests were carried out and what proportion of those came back positive. If you are testing lots of people and only picking up a few positive cases, you can be confident that you are finding most of them. This gives you a low TPR. A high rate means you are missing lots of cases and therefore not doing enough testing to get an accurate picture of what is happening in the country.
This table shows countries such as Hong Kong and New Zealand that are finding almost all their positive cases, through to countries such as Brazil and Mexico, which are doing a lot of testing but are likely to be missing tens of thousands of cases.
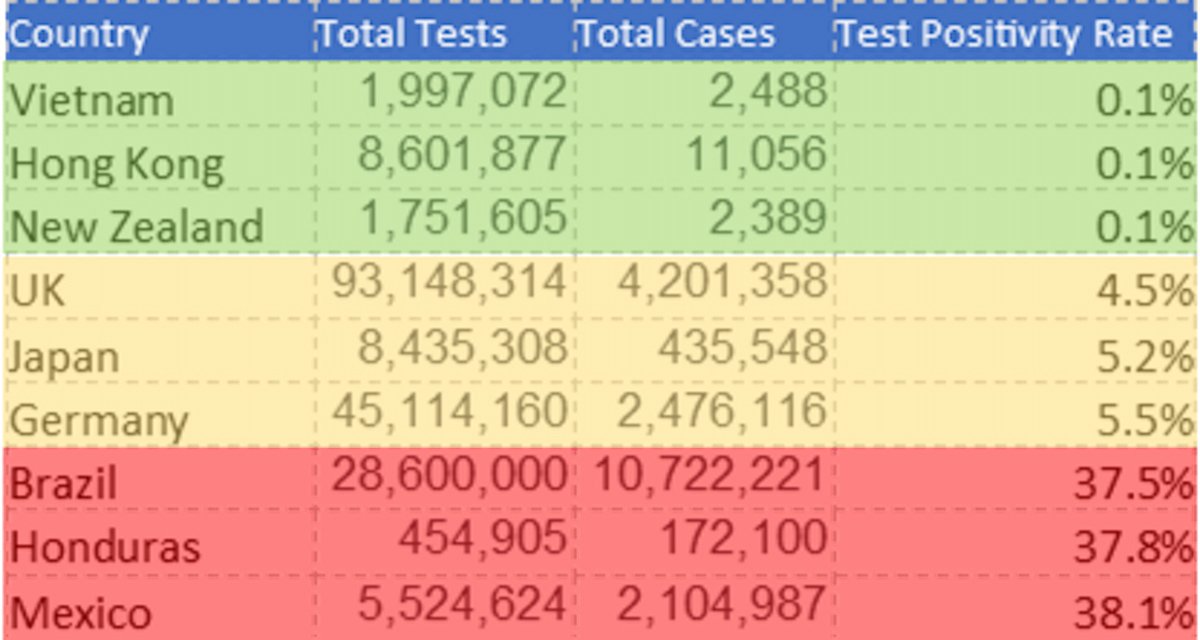
The World Health Organisation (WHO) recommends that no more than 5 per cent of your tests should be coming back positive, to ensure you are finding as many cases as possible. The UK does now fall into this category, which means that although we are undoubtedly still missing cases, we do have a good idea of what our case rate is doing.
“I know people that have tested both negative and positive on the same day, how is this possible?”
It is possible to test negative if the amount of virus present hasn’t reached a certain threshold yet. This is fairly common in the first few days post-infection, so plenty of people test negative and later test positive. If they test positive and then negative, it may be that the level of virus has fallen below the detectable level thanks to the immune system doing its job, or it could be a false negative, which is fairly common, particularly if the swabbing isn’t done well.

“The PCR tests are picking up ‘dead’ Covid-19 virus even when someone is not ill anymore, so it is a worthless test.”
It is true that PCR is very sensitive and may be able to detect fragments of the virus up to a week or two after someone was infected. A positive PCR does not in itself indicate whether the patient is still infectious or not – it simply indicates that RNA from the virus is present. As RNA is not especially stable, PCR will not detect any viral RNA beyond a couple of weeks after an infection.
Ultimately, the PCR test for Covid-19 will only give a positive result if the Covid-19 virus is present. The fact that it may be ‘old’ virus does not detract from how valuable a tool it is in finding people who are infected and stopping them from infecting others.
“PCR tests have been running too many cycles, causing lots of false positives.”
The PCR test involves taking a sample, which may or may not contain genetic material from the SARS-CoV-2, and running it through a series of cycles, each cycle doubling the amount of DNA present in the sample. The mixture also contains a fluorescent dye that only fluoresces when it is bound to DNA. The more DNA present, the brighter the fluorescence. The equipment measures how much fluorescence there is in each cycle, and on which cycle number the fluorescence is first detectable.
The more virus that is present in the sample, the more DNA there is at the start of the PCR, and the sooner it will be detected. Less virus means less DNA in the sample and it will take more cycles to reach a detectable level.
The cycle number at which DNA is detected is known as the Ct value (the Threshold Cycle). The lower the Ct value, the higher the viral load and vice versa. If the sample has a Ct of 25 then there was a lot of virus present in the sample, but a Ct of 38 or 39 means there were only very small amounts of virus in the sample.
There has been debate over whether a high Ct means that the virus is no longer infectious. So should a person have to isolate if their sample has a Ct higher than 39? That is a valid debate to have.
The confusion has come in from people thinking the Ct value and the number of cycles that a lab performs are the same thing. They aren’t. A lab may run their PCR for 50 cycles, but that doesn’t mean it takes 50 cycles before they see a signal. This has led to people who don’t understand PCR trying to claim that labs running a PCR for 50 cycles will only be picking up ‘dead’ viral particles.
It’s also important to reiterate here that you could run a PCR for 60 or 100 cycles and if there is no SARS-CoV-2 virus in the sample, you will not get a positive result. You cannot amplify something that is not there. This has been nicely illustrated by virologist Dr Ian Mackay, who ran a PCR for 55 cycles with one sample known to contain a virus, and multiple samples that did not contain that specific virus. As you can see from the results, only the positive control was able to be amplified.
“Kary Mullis, the inventor of PCR said PCR can’t be used for detecting SARS-CoV-2”
I’ve seen lots of people who want to downplay Covid-19 numbers use this as some sort of argument for why PCR is not a valid way to test people. However, there are a number of flaws in this argument:
- Kary Mullis died in August 2019, four months before the first appearance of Covid-19, making it highly improbable that he would have had an opinion on the use of PCR in diagnosing Covid-19!
- While alive, he had some pretty discredited views. He adamantly denied that HIV caused AIDS, and that is thought to be the basis for the current claims. He did not believe PCR should be used to identify the HIV virus in AIDS patients, as he did not believe the virus was the cause.
- He may have been credited with inventing PCR in the mid-1980s, but that doesn’t necessarily make him an expert on how the technique would develop and what uses it would find. His claims that the technique shouldn’t be used for detecting virus infections hold no more weight than John Logie Baird, the inventor of television, claiming you shouldn’t use it to do your shopping!
- And for a little more context, Mullis spent much of the 1960s and 70s synthesising and taking his own LSD. He was a climate change denier, reported having conversations with a standard extra-terrestrial raccoon, and believed he had been abducted by aliens…
“The virus has never been isolated and therefore does not fulfil Koch’s Postulates”
This claim is routinely made by people who in all likelihood had never before heard of Koch’s Postulates ‒ the criteria designed to establish the link between a microbe and the disease it causes ‒ let alone know what they mean.
These criteria were designed in the mid-1800s, long before the existence of viruses was discovered. Even at the time, Koch himself accepted there were limitations to these criteria, and they did not apply in all cases.
One of the criteria states: “The microorganism must be isolated from a diseased organism and grown in PURE culture.”
Now, this is reasonable if you are looking at bacteria, parasites, and fungi, but viruses are not living organisms and are therefore incapable of being grown in a culture without host cells in there with them!
This has been used by Covid-19 deniers to try and claim that because the SARS-CoV-2 virus has never been grown in a PURE form, it therefore has not been isolated and does not fulfil the criteria to be a disease-forming agent. We know that the virus has in fact been isolated hundreds of thousands of times in the last year. The Next Strain group, who are tracking the evolution of the virus, have isolated it over 20,000 times.
A note on lateral flow tests
These are the ‘rapid result tests’ currently being used in schools and many other areas where a speedy turnaround is helpful. They work in an entirely different way to PCR tests and need a paper of their own. Watch out for it!
Conclusion
In conclusion, there is a lot of misinformation out there regarding the validity of Covid-19 testing. The vast majority of this comes from people with no prior knowledge of how these tests work, and with an agenda to try and downplay Covid-19 cases.
In the end no test is 100 per cent infallible, but PCR is incredibly good at giving a positive result in a Covid-19 patient, and very good at giving a negative result when no virus is present. The timing of the test and quality of the sample taken can impact the result, meaning occasionally a negative test result will be inaccurate. But a positive test result will (almost) never be inaccurate!




