Debunking Covid-19 myths
Myths surrounding Covid-19 are no joke – they are dangerous and hampering our prospects for returning to normality. We are building a comprehensive list of Covid-19 myths and setting the record straight. Researched and collated by Emma Monk
Want to contribute? Do you have a myth you wish to debunk? Please get in touch.

There are some fantastic resources explaining how the vaccines work, which I won’t cover. The AstraZeneca vaccine is explained with great diagrams here, and the Pfizer one here.
1. There have only been 388 Covid-19 deaths among the under-60s in the UK.
2. Covid-19 only kills people who were about to die anyway.
4. Why are there many videos of empty hospitals?
5. Why are the Nightingale facilities being dismantled and closed?
6. Hospitals are always busy in the winter and none of them have reached full capacity yet?
7. How do we know whether people have died FROM Covid-19 as opposed to just WITH Covid-19?
10. In 99.9 per cent of cases, people’s immune systems deal with the virus perfectly well.
11. People die all the time. It’s a fact of life.
12. Why enforce masks when they’ve been proven not to work?
13. Masks do more harm than good.
14. I know someone who always wore a mask and they still caught Covid-19, so they obviously don’t work.
16. Lockdowns have completely trashed the economy.
18. But what about Sweden? They didn’t lockdown and they were ok.
19. Lockdowns have stopped us from being able to develop herd immunity.
20. Lockdowns have huge impact on mental health.
21. Lockdowns have caused a massive increase in self-harm and suicides.
26. The vaccine trials have been too quick – no one knows what the long-term side effects will be.
27. The vaccines have been developed too quickly – they must have cut corners.
28. The Covid-19 vaccines are killing people.
29. The Covid-19 vaccine causes infertility
30. The Covid-19 vaccine will alter your DNA.
31. The Covid-19 vaccine will give me Covid-19.
32. People are suffering all sorts of horrendous side effects after having the vaccine, which the government is trying to keep hidden.
33. The COVID-19 vaccine contains microchips.
34. The Covid-19 vaccine contains cells from aborted foetuses and monkey DNA.
1. There have only been 388 Covid-19 deaths among the under-60s in the UK.
This is a truly callous claim. It came from a report in various newspapers stating “388 people aged under 60 with ‘NO underlying health conditions’ have died of Covid-19 in England’s hospitals” in December 2020.
However, the list of pre-existing health conditions covered anything from autism to asthma, learning difficulties to angina, and fractured arms to glaucoma.
To discount the death from Covid-19 of someone who is autistic as a means of trying to minimise the severity of the disease is quite frankly sickening; as is discounting the death of anyone over 60. To date, over 80,000 people have died in the UK as a direct result of Covid-19, all leaving behind sons and daughters, brothers and sisters, friends, partners and loved ones. Discounting their deaths because they had learning difficulties or because they are over 60 is a dangerous path on which to travel. Back to the menu…
2. Covid-19 only kills people who were about to die anyway.
This is related to the previous claim and is regularly used to downplay the numbers. There are two very stark pieces of evidence that easily disprove this claim.
First – excess deaths. A five-year average of the number of people who die each week, month or year can be compared to the number of deaths in the same time period this year. The cause of death is irrelevant; it is simply a measure of how many more people died than you would have expected in a normal year. In 2020, around 73,000 more people died than the average of the previous five years. That’s 14 per cent above the average – the highest excess death number we’ve seen in the UK since 1940.
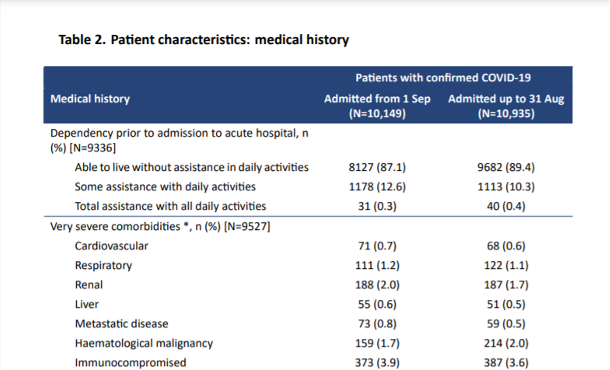
Second – intensive care unit (ICU) statistics. The Intensive Care National Audit and Research Centre (ICNARC) produces a regular report (here) on the characteristics of patients in intensive care in the UK. These are the most severely ill patients, with around 30 per cent not surviving. Of these patients in ICU, nearly 90 per cent were living fully unassisted lives prior to admission, with less than 0.5 per cent needing round-the-clock care. Less than 10 per cent were considered to have severe comorbidities (underlying health factors). These were people living fully active lives before contracting Covid-19.
3. In September, Covid-19 was the 19th highest cause of death. 19th!! Why are we not addressing the 18 others before it?
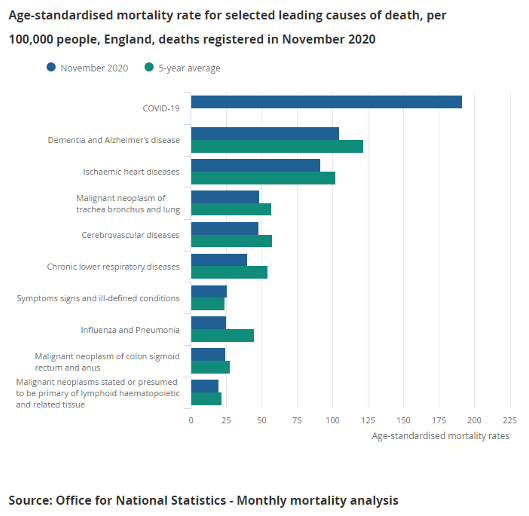
In September, deaths from Covid-19 were low following the initial lockdown and the warm summer months. Unfortunately, that was the calm before the storm. According to the Office for National Statistics (ONS): “The coronavirus (Covid-19) was the leading cause of death in November 2020 for the first time since May 2020 in both England (accounting for 18.1 per cent of all deaths registered in November) and Wales (21.6 per cent of all deaths); looking at all deaths registered in January to November 2020, Covid-19 was the second most common cause of death in England and Wales (after dementia and Alzheimer’s disease).”
And we are still addressing the other causes. But none of them have the infection rates and mortality rates of Covid-19. They continue to be treated (as long as hospitals have capacity), as they have always been. Back to the menu…
4. Why are there many videos of empty hospitals?
Because many hospitals have had to close wards to increase their ICU capacity. An empty ward simply shows that staff have had to be deployed elsewhere and so the ward cannot remain open.
[Ed: In addition, Covid-deniers have been posting stock images of empty wards, some of them not even in the UK, to claim that Covid-19 is a hoax.]
5. Why are the Nightingale facilities being dismantled and closed?
Because, unfortunately, they were only ever a nice idea or PR stunt (depending on your viewpoint!). They were simply buildings with beds and some ventilators, but they were never equipped with staff – making them unusable. For a patient to be transferred there they needed to come with staff – which hospitals could not spare. Back to the menu…
6. Hospitals are always busy in the winter and none of them have reached full capacity yet?
Yes, hospitals are often busy in the winter, but NHS staff are reporting that they’ve never been hit like this. The capacity figures can be misleading as they are often quoted as a percentage of the available beds. Most ICUs have doubled or tripled their capacity over the last few months, by closing down other departments, theatres, etc and re-deploying staff. So, a hospital that usually has 50 ICU beds may now have 150 beds. If 135 of those beds are full, this is reported as being at 90-per-cent capacity – a figure seen regularly in winter – when actually they are at 270-per-cent capacity compared to normal.
The Financial Times statistician, John Burn-Murdoch has produced a very good animation comparing this winter to previous ones. The numbers for this winter are literally off the scale compared to the last six winters. Back to the menu…
7. How do we know whether people have died FROM Covid-19 as opposed to just WITH Covid-19?
There are many claims that people are dying following a positive Covid-19 test from causes unrelated to their Covid-19 infection.
Now, obviously, there will be a tiny number of people for whom that is the case. But the overwhelming majority of people who die within 28 days of getting a positive Covid-19 test are dying as a direct result of contracting Covid-19.
We have multiple sources that show this to be true:
- Excess deaths have mirrored the rise and fall in Covid-19 deaths pretty accurately, suggesting that these excess deaths are the result of people dying from Covid-19. If these people were dying from ‘regular’ causes and just happened to have had a positive Covid-19 test, there would not have been any excess deaths.
- Doctors are well trained in diagnosing disease and are very good at using all the information available to them to make the call on cause of death. When they fill out a death certificate, they write down the event that directly led to death, but they can also write down other contributing factors, including the presence of a positive Covid-19 test and other underlying factors. If a patient dies from cancer, while being positive for Covid-19, the cause will be cancer with Covid-19 mentioned. If a patient undergoing cancer treatment contracts Covid-19 and dies from the effects of Covid-19 (inability to breath, etc), then the cause of death is Covid-19 with cancer mentioned.
- The ONS analyses all these death certificates, looking at the direct cause and the other factors mentioned, and differentiates those who have died WITH and those who have died FROM Covid-19. This data is released every week, and shows that between 80 and 90 per cent of deaths where Covid-19 is mentioned on the death certificate are the direct result of the Covid-19 infection.
8. Why are deaths being marked as Covid-19 up to 28 days after a positive test if we only have to isolate for 10–14 days after testing positive?
Back in the spring, the easiest and quickest way to collate daily data on Covid-19 deaths was to compare anyone who had died with the database of those who had had a positive Covid-19 test. As testing was only being done on people with severe symptoms at that time, it was a reasonable assumption that those who tested positive and then passed away died from Covid-19.
However, by the summer, as fewer people were dying from Covid-19, and more people were ending up on the positive-test list, it became more likely that someone could die from something unrelated to a Covid-19 test that they may have had months before.
A review of the available data showed that 88 per cent of Covid-19 deaths occurred within 28 days of a positive test (96 per cent occurred within 60 days). The 28-day timescale was also being used in other countries for their reporting, so it was chosen as the UK cut-off.
The chance of anyone testing positive for Covid-19 and then dying of something unrelated within four weeks is vanishingly tiny. However, we do know that the 28-day cut-off underestimates Covid-19 deaths.
For those who do not need hospital treatment, the 10–14-day isolation covers the time when they are most infectious and so should stay at home. Back to the menu…
9. Why, when they have already been caught in August exaggerating Covid-19 death figures, do you not think they’d do it again?
August was when they made the decision to introduce the 28-day cut-off, which led to a number of deaths being removed from the official statistics. As we know from ONS data based on death certificates, the running total of ‘official’ Covid-19 deaths was already lower than the number of actual Covid-19 deaths. This decision actually made this problem even worse. So, far from ‘being caught exaggerating the figures’, they were making their underestimates even more pronounced. Back to the menu…
10. In 99.9 per cent of cases, people’s immune systems deal with the virus perfectly well.
I’ve seen many people trying to claim that over 99.9 per cent of people who catch the virus survive, but, first, the figure is simply not true and, second, dying is not the only adverse outcome.
Of those who contract Covid-19, around 1 per cent will die from it. This varies greatly depending on your age (over-80s have a 15-per-cent chance of dying, with the percentage for under-40s being very low).
However, a further 5 per cent require hospitalisation, and with treatment will survive. These patients would be unlikely to survive without hospital treatment, so the mortality rate increases as hospitals become overrun.
As well as simply looking at death or survival, the long-term health effects of Covid-19 need to be considered. According to the ‘ZOE COVID Symptom Study’: “Long Covid-19 affects around 10 per cent of 18–49-year-olds who become unwell with Covid-19, rising to 22 per cent of over-70s”, which is likely to add an increased burden to our health system and economy for months and years to come.
So, deaths are not the only thing to worry about. But even if they were, a 1-per-cent mortality rate in a highly transmissible disease is very much a reason to take it seriously. 1 per cent of the UK population would be 680,000 deaths … Back to the menu…
11. People die all the time. It’s a fact of life.
That’s true, but the sheer number of people who have died in the last 10 months from Covid-19 is hard to imagine. 80,000 people in the UK have died from Covid-19 since February 2020. That is the capacity of the Olympic Stadium.

Since 1900, only two years have seen more than 600,000 deaths in the UK – 1918 (the year of the Global Flu Pandemic, commonly and unfairly known as ‘Spanish’ flu) and 2020. Back to the menu…
12. Why enforce masks when they’ve been proven not to work?
Masks have not been ‘proven not to work’. A review of over 140 studies and academic papers found overwhelming evidence to support the wearing of masks to prevent the spread of Covid-19. It found:
- If at least 70 per cent of people wore masks, modelling suggests that combined with contact tracing, that would be sufficient to stop the epidemic growing.
- People are most infectious before developing symptoms making widespread mask use, whether you have symptoms or not, absolutely vital.
- All types of material are helpful at preventing the spread of the disease from an infected carrier, although some are better than others.
- Masks offer some protection to the wearer, although the primary benefit is in preventing infectious people from spreading the virus.
They also found an American economic analysis suggesting universal mask wearing could add 1 trillion dollars to the US GDP. Back to the menu…
13. Masks do more harm than good.

There have been suggestions that mask wearing would lead to people getting complacent about other measures such as distancing and handwashing. Similar arguments about risk behaviour were made about motorbike helmets, seatbelts, and ski helmets when they were introduced and were equally unfounded. Observational data during the pandemic has shown that mask wearers are better at hand hygiene, distancing and reduced face touching. There is also data to suggest that mask wearing acts as a cue to others to keep their distance.
There has also been a suggestion that masks can cause bacterial pneumonia, but this is simply not true. There appear to be no records showing it happening anywhere, despite the claim, and doctors have explained that the only thing that ends up on your face mask is what you breath out. For your exhaled breath to contain pneumonia-causing bacteria it would have to be in your lungs already. Back to the menu…
14. I know someone who always wore a mask and they still caught Covid-19, so they obviously don’t work.
The primary benefit of mask wearing is to protect those around you. There has been shown to be some protective effect on the wearer, but not as strong as the effect they have on protecting those around you.
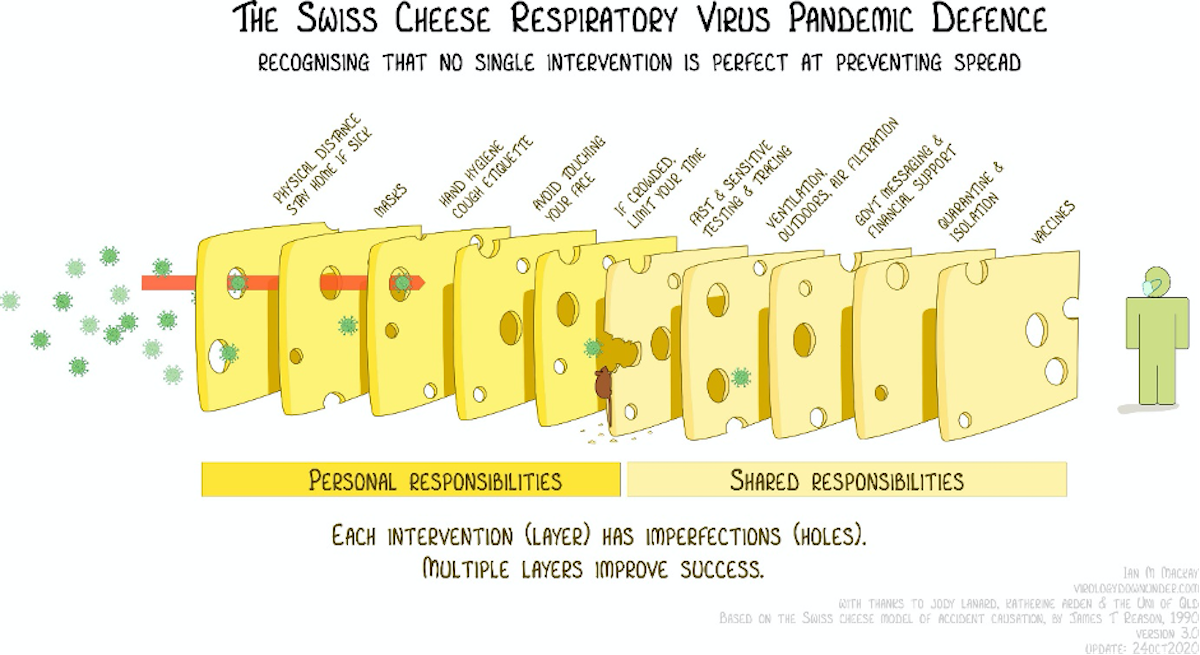
No measure will be 100 per cent effective in stopping the pandemic, but multiple measures used together are our best shot.
15. Lockdowns don’t work.
Covid-19 can only spread by people mixing. It cannot spread without a human involved. So just on a purely logical level, staying at home as much as possible will prevent the virus from spreading.
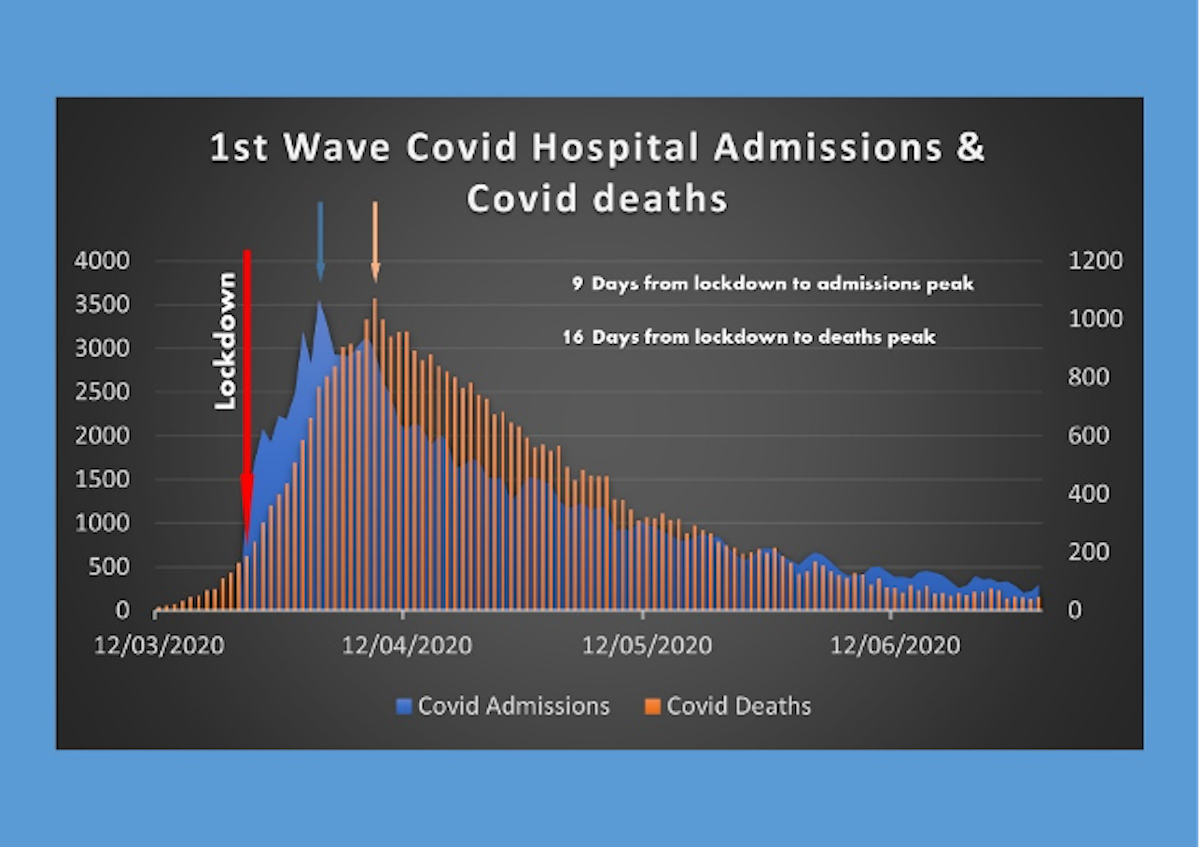
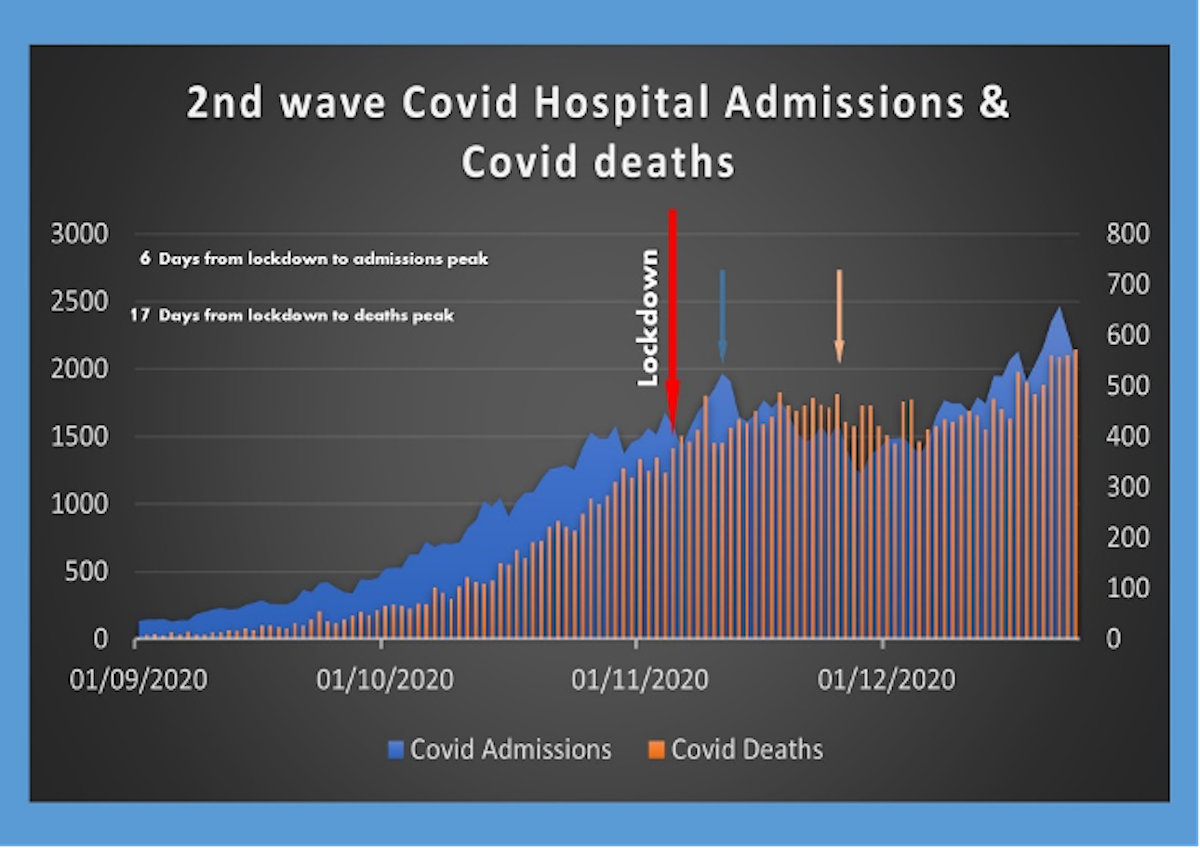
There is a time lag between restrictions being put in place and the effects being seen in either hospital admissions or deaths recorded. It takes up to 14 days for symptoms to appear (average length five days after infection), an average of 3-10 days between symptoms and hospital admissions, and an average of two weeks between symptoms and death.
Looking at the first lockdown in the spring, you can see that hospital admissions started falling after around 9 days, while deaths started falling about a week later. This is entirely in line with the timings you would expect to see if it were the lockdown restrictions that were limiting cases.
The second lockdown in November was much looser, so did not have the same dramatic effect that the first lockdown did. The time lags were still indicative of the restrictions having a significant effect on slowing the spread of Covid-19. Unfortunately, the effects were quickly wiped out by shopping and mixing in the run up to Christmas.
16. Lockdowns have completely trashed the economy.
Lockdowns do have a major effect on the economy, as retail, manufacturing, hospitality, live events etc., all have to stop.
However, it is not as straightforward as that. Had there not been a lockdown, retail, hospitality and live events would still have been hit hard by people choosing to stay at home for fear of catching the virus, and by people being unable to work through sickness, and sadly, death.
One of the arguments put forward to delaying lockdown back in spring was to ‘keep the economy going as long as possible’, but unfortunately this argument didn’t play out well.
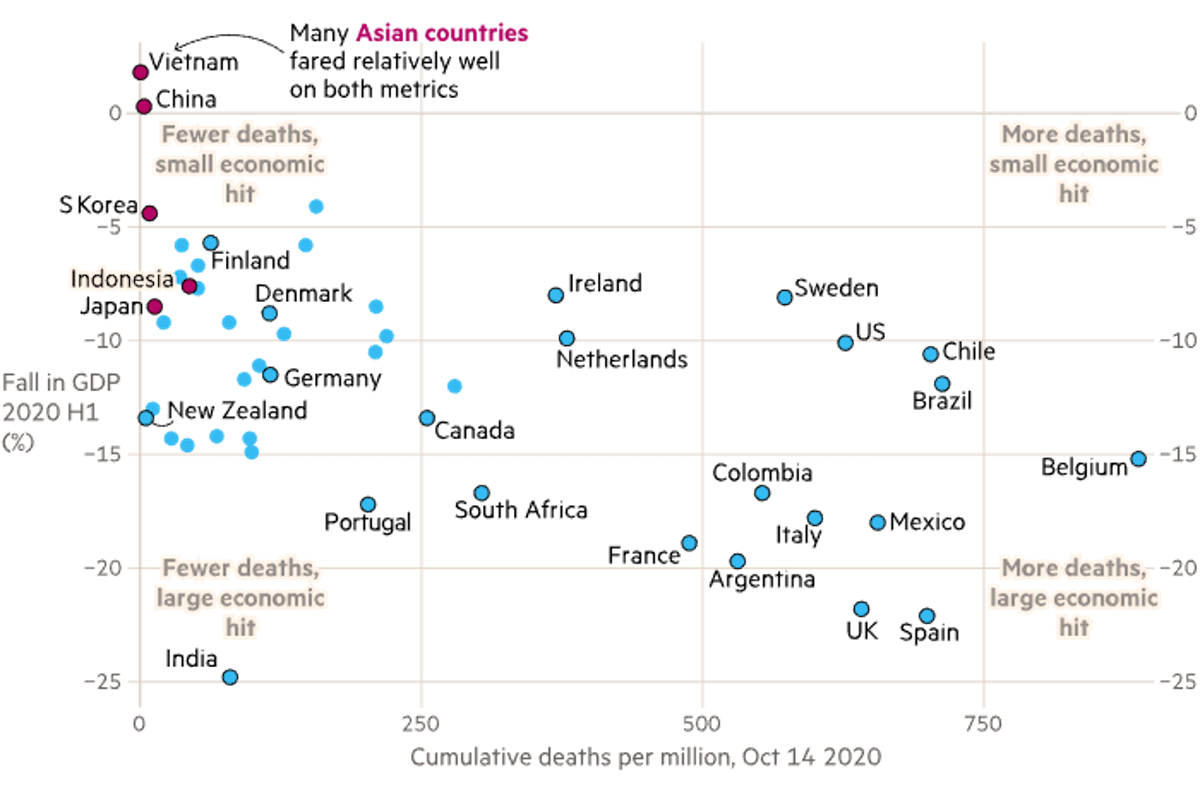
Analysis has shown that the countries that got the spread of the virus under control the most effectively, often by locking down hard and fast, ended up with a far lesser impact on their economy. The UK was one of the worst performing in both the economy and number of deaths, as shown in this graph from Covid-19: The global crisis — in data.
The argument that you have to balance health with wealth is a false dichotomy. A healthy population is intrinsically linked to a healthy economy and you cannot have one without the other. Back to the menu…
17. Scientists forcing lockdowns on us predicted there would be 500,000 deaths in the UK, but they were wrong – we never should have locked down based on their data.
Neil Ferguson published a modelling report in March that showed if we took no steps at all to curb the spread of the virus, we could see 550,000 deaths over 2 years as a result. The point of the modelling was to decide which steps would be most effective in suppressing the virus and saving lives. Many steps were then taken to limit the spread, including social distancing, encouraging handwashing, closing mass gatherings, closing schools and other lockdown measures. All these interventions played a role in slowing the spread of the virus, limiting the number of people who became infected and therefore the number of people who died.
The fact that 550,000 people did not die does NOT mean those steps were not needed. It shows the opposite. Back to the menu…
18. But what about Sweden? They didn’t lockdown and they were ok.
Sweden chose a quite different route to dealing with the pandemic and was hailed as a success by many lockdown sceptics early on. They chose to ban large gatherings, close their airports, move high schools and universities to distance learning, and encourage working from home, but kept junior schools, non-essential shops, bars, and restaurants open, albeit with social distancing guidelines in place.
Unfortunately, Sweden ended up with one of the highest per capita death tolls in the world AND took a greater financial hit than other similar economies.
Authorities in Sweden have been widely criticized, with some apologising for failing to protect the elderly and nursing home residents. Back to the menu…
19. Lockdowns have stopped us from being able to develop herd immunity.
Some people were calling for a ‘herd immunity’ strategy from early on. The UK and Sweden appear to have been the only countries planning to follow that path.
The idea was to protect the vulnerable and allow the virus to spread through the rest of the population, allowing them to build up immunity. If enough people have immunity, the population is said to have ‘herd immunity’ – where people are protected by the fact that others are immune, and the disease won’t spread.
However, there has never been a human virus that has reached a high enough level of herd immunity to protect the vulnerable, without a vaccine. Even if it were possible, it would require at least 70 per cent of the population to have been infected and developed immunity. As this virus has a mortality rate of one per cent, it would lead to around 500,000 people dying in the UK alone. The evidence on whether you end up with long term immunity from contracting the disease is also not clear.
Sweden hoped that their light touch lockdown would have at least increased their levels of immunity, however widespread studies of antibody levels have shown that only 17 per cent of residents in Stockholm had immunity by the summer, with levels of only four per cent elsewhere in Sweden. London also showed around 17 per cent with five per cent elsewhere in England. Back to the menu…
{kind=link}
20. Lockdowns have huge impact on mental health.
Most people are justifiably concerned about the effects of lockdown on the mental health of the population. The ONS (Office for National Statistics) routinely survey people to get a snapshot of how the nation is feeling. It is clear that people are feeling less happy, less satisfied with life and more anxious than they were in February 2020. What is less clear is whether this change is as a result of the lockdowns themselves or a result of the pandemic in general. For example, anxiety levels were at their highest in March, improving during the summer. However, the lockdown in November did not appear to impact the levels at all. They have gone up again at the start of January, but whether that is down the worsening news regarding new variants, overcrowded hospitals or the prospect of the lockdown, is hard to tell.

21. Lockdowns have caused a massive increase in self-harm and suicides.
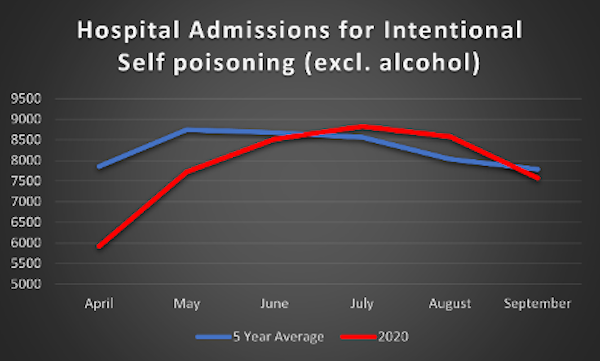
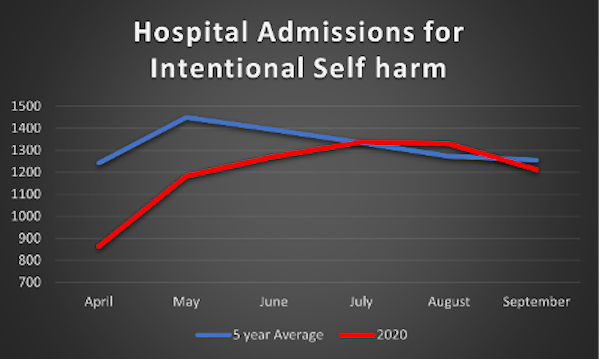
There have been concerns regarding the levels of self-harm and suicides that could be caused by lockdowns, with many mental health organisations warning of severe impacts on mental health from loneliness, isolation and money concerns. However, it is hard to quantify these effects. Data shown here looks at the number of hospital admissions for self-harm and self-poisoning each month between April and September 2020 compared to the average for each month in the last 5 years. April, May and June (during lockdown) all saw lower than average numbers, with numbers being slightly higher than average during the summer months. This does not support the theory that lockdowns caused an increase in self harming.
A Study by Manchester University looked at suicide figures from established ‘real-time surveillance’ systems in several parts of England, comparing the months pre-lockdown (January-March 2020) to post-lockdown (April-August 2020). The average number of suicides per month varied but there was no evidence of a rise post-lockdown. They caveated the report by saying that the study only covered parts of England (population of around nine million), and they could not rule out a future rise as the economic impact of the pandemic continues to take its toll.
A British Medical Journal editorial examined the available data from across the world relating to suicide rates during lockdown and concluded “Nevertheless, a reasonably consistent picture is beginning to emerge from high income countries. Reports suggest either no rise in suicide rates (Massachusetts, USA; Victoria, Australia; England) or a fall (Japan, Norway) in the early months of the pandemic. The picture is much less clear in low- income countries, where the safety nets available in better resourced settings may be lacking.”
There is absolutely no question people are suffering as a result of the lockdowns. But it is really important to also understand that without the lockdowns, the suffering may have been just as much of a problem as many more people would have lost loved ones, and the economy would likely have been equally badly hit (see section above on economy). Back to the menu…
22. Lockdown meant hospitals stopped treating anyone else. They were only interested in Covid-19 Patients.
This is a common misconception. The hospitals did not ‘close’ during lockdown. They continued to treat anyone who needed emergency treatment, as long as they had the staff and ICU (Intensive Care Unit) capacity. Non-emergency, routine surgery needed to be cancelled as staff were deployed to other areas of the hospital. Surgery always comes with a risk of requiring intensive care, so cancelling these types of surgeries ensured the ICUs were available for critical patients.
Once a hospital reaches capacity, whether with Covid-19 patients, flu patients, or stroke and heart attacks, then the ability to treat anyone disappears, regardless of the need. So, an ICU full of Covid-19 patients means there is no room for the car crash victim or meningitis case. This is why the primary reason given for lockdowns is to prevent the hospitals becoming overrun with Covid-19 patients. Keeping numbers down is the best way to save lives from any cause – not just from Covid-19.
Dr Pimenta illustrates it nicely:
It is worth noting that in countries which dealt swiftly and successfully with their Covid-19 outbreaks, access to healthcare for other reasons was not impacted on the scale we have seen in the UK. In May, the World Health Organisation (WHO) sent a survey to 194 ministries of Health, of whom 163 responded. The results showed that less than 50 per cent of countries saw disruption to their cancer services, emergency dental care, diabetes care, asthma services or palliative care. In the UK, the fifth richest nation and the second most pandemic prepared country (on paper!) we saw widespread disruption to our health services. This is more a reflection of our poor response and long-term poor funding of our health service, than a direct consequence of lockdown. Back to the menu…
23. Lockdown caused more deaths than Covid-19.
Some headlines have claimed that the lockdown itself was going to cause ‘more deaths than covid-19’. However, there does not appear to be any factual basis to these claims – other than the opinion of the journalists!
Many papers ran with the headline in July that an ONS report had estimated that lockdown would result in an additional 200,000 deaths. However, when looking at the report itself, this is only half the story. It estimates the number of deaths due to delayed healthcare, suicides, domestic abuse, people being scared to go to hospital etc., following a lockdown. These were around 200,000 in the long term, in addition to the 45,000 predicted Covid-19 deaths at the time. Then, the report compared this to the number of deaths estimated if no lockdown had been implemented. These were estimated at 450,000 Covid-19 deaths and more than 1,000,000 deaths as a direct result of people not being able to access hospital care due to over-run hospitals.
So, although the effects of reduced hospital care during lockdown could lead to significant lives lost in the future, NOT locking down would likely have led to around five times that number in non-Covid-19 deaths, and double that number in Covid-19 deaths. Back to the menu…
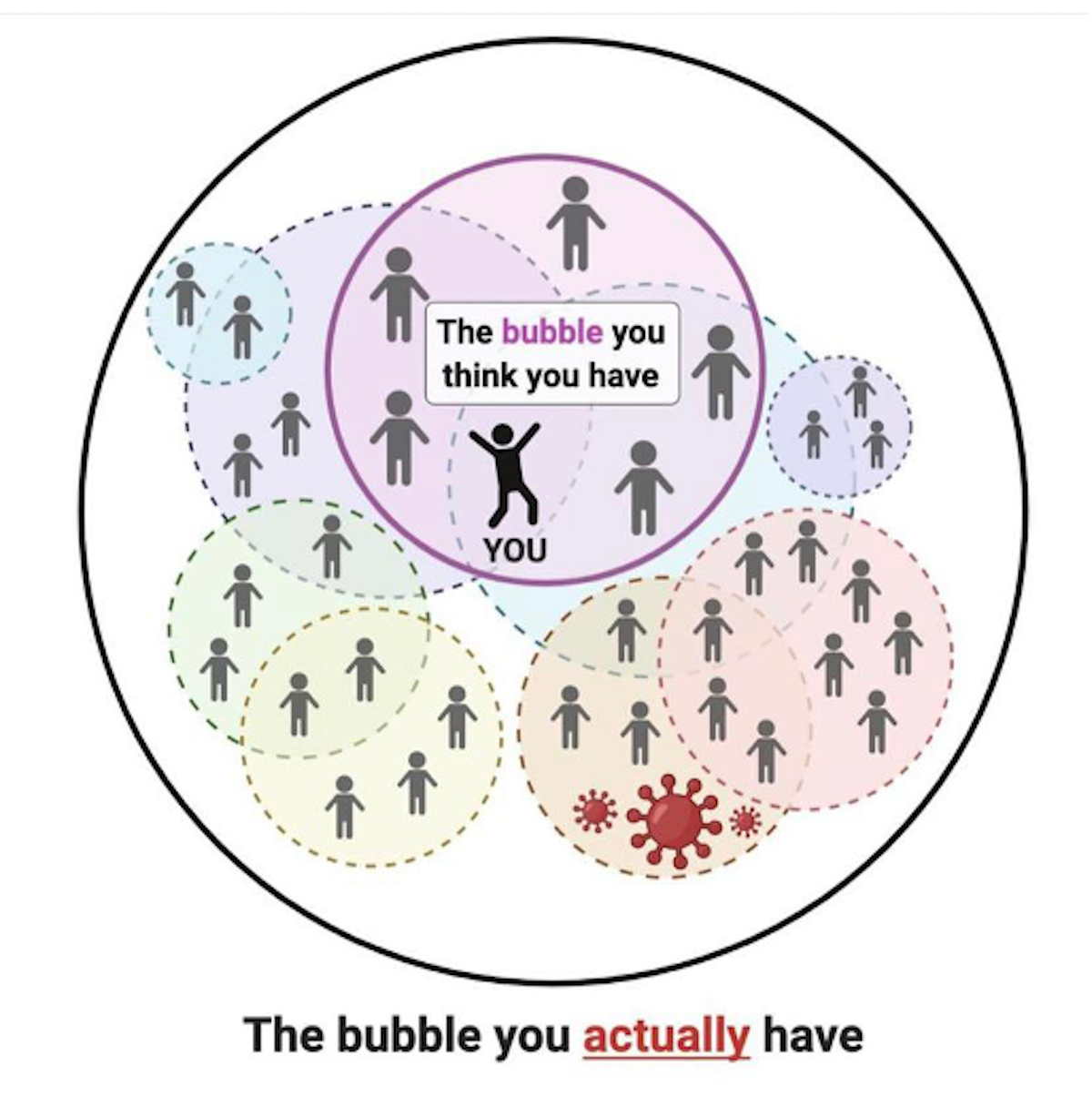
24. Can’t we just protect the vulnerable and let everyone else live life as normal, like they suggested with the Great Barrington Declaration?
The Great Barrington Declaration was written by 3 scientists and funded by right wing climate change denier Charles Koch and supposedly signed up to by 8000 scientists. However, many of these have been proven to be fake signatories, including Dr Sciency McScienceface and Dr Wibbleton Wibbler! Anyone could sign it with no authentication or confirmation of their credentials needed. It has been widely discredited by the scientific and medical communities.
The idea was a vague notion that you could somehow lock away the ‘vulnerable’ while allowing everyone else to carry on as normal. There were no suggestions on how this would actually work in principle. Our lives are highly interconnected, as illustrated below, with every visit to buy food, collect medicine or receive care leading to the vulnerable coming into contact with those ‘carrying on as normal’.
There are just over 10 million people in the UK in the extremely high risk categories (over 70s and Extremely Clinically Vulnerable), with a further 17.2 million considered moderately high risk (50-70 year olds and those with underlying conditions that put them ‘at risk’ from Covid-19). The idea that 14-40 per cent of the UK population could be kept completely shielded from the rest of the population is just simply unworkable. Not to mention the massive hit the economy would take from the working aged vulnerable people being unable to work, or any of the vulnerable being unable to go to garden ientres, shops, restaurants etc.
It is also worth mentioning that although the risk of death from Covid-19 in the younger age groups is low, there is a lot of evidence coming out now of long-term health risks, known as ‘Long-Covid’, associated with even mild cases of the disease. The long-term effects on the healthcare system and the economy are likely to be significant, and the more you allow the virus to spread, the more people are likely to end up in this category.
In addition, the more people you allow to contract Covid-19 the higher the chances of new, more transmissible (catching) strains of Covid-19 developing, as we have seen with the new B117 variant.
25. If vaccines are so ‘safe’ then why are the vaccine companies not responsible for paying for compensation, like they are for medicines?
In the 1970s a little girl developed polio after taking the live polio vaccine. This was a known but very rare possibility (far less likely than her chances of developing polio without the vaccine). However, the doctor had not warned her father about it, so the father sued the company and won his case.
This set a precedent for people to sue vaccine makers if they believed they had been affected adversely by the vaccine. Unfortunately, it is impossible to prove a negative, so as long as the symptom developed shortly after the vaccine was given, the vaccine was assumed to be the cause.
Unsurprisingly, this led pharmaceutical companies to become reluctant to develop vaccines, as the huge legal costs of compensating anyone who claimed a vaccine injury, added to the immense costs of developing the vaccine to begin with, made it financially unviable. So governments stepped in and set up vaccine-injury compensation programmes to deal with the payments, allowing the drug companies to get back to developing much-needed vaccines.
This has led to an inflated public awareness of ‘vaccine injury’, far more than any fears or discussion surrounding medicinal side effects. Despite all the claims in the US, in around 70 per cent of the compensation cases the committee agreed a settlement “in which they had not concluded, based upon review of the evidence, that the alleged vaccine caused the alleged injury.”
For some perspective: in the US (a very litigious society) around 300 million doses of vaccines are administered every year, with around 300 successful claims made to their compensation programme. Only around 30 per cent have shown any evidence of a link, suggesting around one in 4.5 million vaccinations result in injury. This is a vanishingly tiny risk, compared to the risk of contracting the diseases the vaccines are preventing. Back to the menu…
26. The vaccine trials have been too quick – no one knows what the long-term side effects will be.
There are two types of potential ‘long-term side effects’: a reaction to the vaccine that has long-term lasting effects, or an effect that won’t been seen for a long time after the vaccination occurs. The former would be picked up by phase three clinical trials, the big studies where thousands of volunteers receive either the vaccine or an inactive placebo. These trials allow the effects of the vaccine to be compared to those who didn’t receive the vaccine, as well as being able to check for any side effects, which would develop shortly after the vaccine was given. Side effects not seen when thousands of people have received the vaccine will be very rare.
The Pfizer/BioNTech trials included 43,000 volunteers and the AstraZeneca trials included 20,000 volunteers, and in both cases the only side effects seen were common vaccine reactions such as headache, sore arm, and tiredness.
Between those trials, and since starting to vaccinate the public, millions of people have now received the vaccine and so far, there have been no major adverse events. So if there is the possibility that one of these vaccines will cause a long-term side effect, it will be a one in a multiple million chance of happening. This should certainly not be a reason to risk catching Covid-19, which has up to a one-in-10 chance of long-term health problems.
As for the second type of side effect – one where you don’t develop symptoms until years after the vaccine – that has only ever been seen with one vaccine: the chickenpox vaccine. The nature of that vaccine means that in rare cases the live attenuated virus (modified virus that can trigger the immune system but is unable to cause disease) can lie dormant and, years later, lead to cases of shingles. It should be noted that getting chickenpox itself is far more likely to lead to the development of shingles in later years.
None of the Covid-19 vaccinations being developed involve this type of vaccine, so there simply isn’t the possibility that this will happen.
So to sum up, if there were to be any long-term side effects of the Covid-19 vaccines, we would have seen them during the trials, or else they are so rare that they should not affect your decision to vaccinate. Back to menu…
27. The vaccines have been developed too quickly – they must have cut corners.
The vaccines have been through the same rigorous clinical trials as any other vaccine and have been proven to be safe. Tens of thousands of volunteers (and now hundreds of thousands of people a day) have had the vaccines and there has been no evidence of any major safety issues. Issues with vaccine safety are generally seen within days or a few weeks of having the vaccine and, so far, none have been reported.
Some people are concerned by how fast these vaccines have been developed, rightly questioning: how come it has happened in less than 12 months when it usually takes years? The answer is vast sums of money, scientific collaborations, more people researching them than ever before, the high prevalence of the virus in the community, and the unprecedented decision to make the vaccines before the trials were complete, so they would be ready to go.
Vaccine trials usually take years because each step happens after the next one: research, followed by getting authorisation to run a trial, followed by recruiting patients, followed by waiting for enough people to be exposed to a disease to see if the vaccine is working, followed by analysis, followed by reporting, followed by more authorisations, followed by finally being allowed to make and use the vaccine. In this case, the number of volunteers, the amount of virus circulating, the money and desire to find a vaccine haven’t been in short supply, which have made all these steps happen faster, but no less rigorously. Back to menu…
28. The Covid-19 vaccines are killing people.
In early January 2021, reports came out of Norway that 33 people in care homes had died within a week of receiving the Pfizer vaccine. This understandably caused a scare in the press. However, the Norwegian Institute of Public Health and the WHO (World Health Organisation) have both confirmed that there was no link between the vaccines and the deaths. 55,000 elderly people in Norway had received the vaccines at that point. 45 people in that age group die every day in Norway, meaning 33 deaths out of 55,000 people vaccinated is not unexpected.
During clinical trials, there were two deaths in the Pfizer vaccine group (compared to six in the placebo group), both of which were investigated and found to be unconnected to the vaccine.
According to the American VAERS (Vaccine Adverse Event Reporting System), a site where you can register any side effects (‘Adverse Events’) you believe were caused by the vaccine (from a sore arm right through to death). Of the 21 million US citizens to receive at least one dose of either the Pfizer or Moderna vaccine by the middle of January, only 196 deaths were reported. It is important to note that each of these deaths is then investigated further, to establish whether the death is a result of the vaccine or not. So far there have been no deaths attributed to the vaccine.
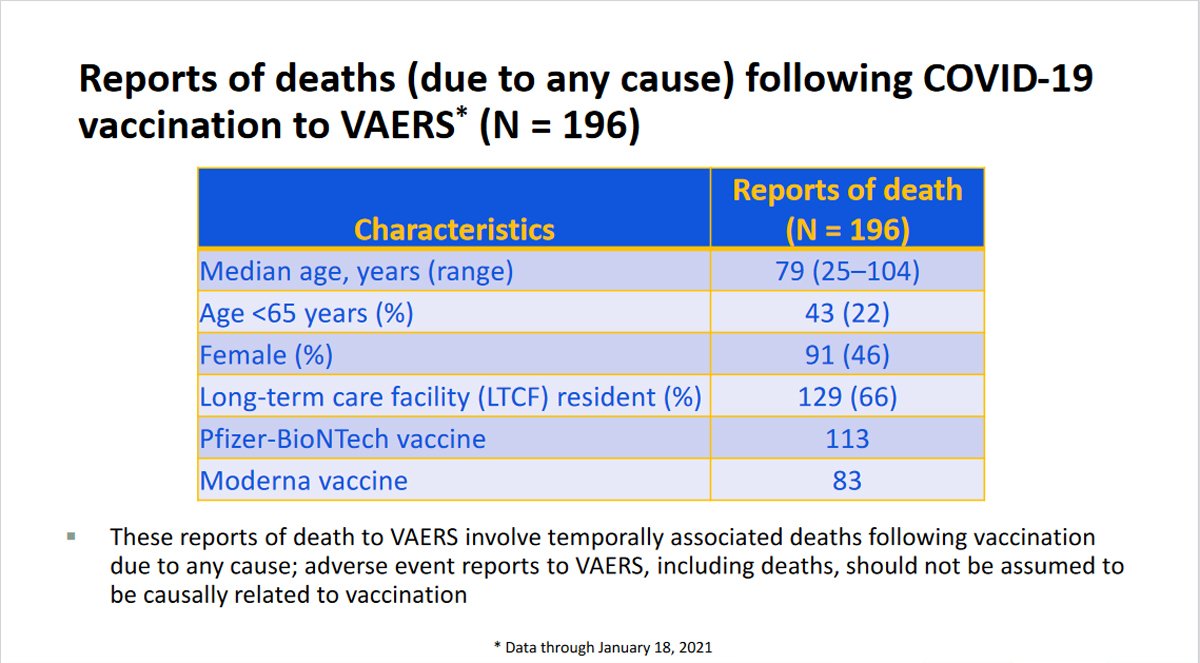
Of the 196 deaths reported, 129 took place in care homes. Based on the age profile of the residents, and the number who were vaccinated, you would statistically expect 11,440 deaths in the timeframe of the post vaccination period, so 129 deaths being reported should not be cause for alarm. It is also interesting to note that mortality in the vaccinated residents of care homes was lower than the unvaccinated residents in the same care homes, and also lower than in the care homes yet to be vaccinated.
In the UK, we see around 1000 deaths each day in the over 80s and the under 80s in care homes and over 80s in the community. Given that this is the age group we are vaccinating first, it is extremely likely that we will see deaths following the vaccination purely by chance, and so caution should be used if you hear stories of people dying after receiving the vaccine. Back to menu…
29. The Covid-19 vaccine causes infertility.
Claims were made that the vaccine targeting the Covid-19 spike protein would also train your body to attack syncytin-1, a protein found in the placenta, because they shared a short amino acid sequence (amino acids are the building blocks of proteins). This would lead the immune system in pregnant women to attack the placenta, leading to miscarriage, and prevent any future pregnancies.
The claim is totally unfounded on multiple levels. Firstly, the shared sequence is so small it is like suggesting that the fact you have the number seven in your phone number means anyone dialling an 11-digit number with a seven in it will connect to you! If you were to compare the sequence of the spike protein to any protein in the human body you will, by chance, find some parts that match. But there is no evidence that Covid-19 antibodies are targeting every protein in your body – if that was the case then infertility would be the least of your worries!
And secondly, if antibodies to the spike protein were causing infertility, you would expect infertility to result from contracting the disease itself. Millions of people across the world have now had Covid-19 and there is no evidence at all that fertility has been affected. We also know that in the Pfizer trials, 12 vaccine volunteers got pregnant, compared to 11 in the placebo group.
Of the 21+million people who had received at least one dose of either the Pfizer or Moderna mRNA vaccines in the USA by late January, more than 15,000 had reported a pregnancy to the vaccine monitoring body, so it’s pretty clear the vaccine is not causing infertility.

30. The Covid-19 vaccine will alter your DNA.
This is simply not true. In order to do that, the mRNA would need to enter the nucleus of the cell (where your DNA is stored), which it can’t do without a ‘nuclear access signal’, which it doesn’t have. Even if it did get in (which it can’t), it would then need to be turned into DNA, which needs something called ‘reverse transcriptase’, which it doesn’t have. And even if it did get in (which it can’t) and turned itself into DNA (which it can’t), it would then need something called ‘integrase’ to insert itself into your DNA, which – you guessed it – it doesn’t have!
Imagine your DNA is a recipe book for how to make every protein in your body. mRNA is like a photocopy of the recipe for the protein you want to make. Photocopies are made all the time and fed into ‘machinery’ that can read the recipe, and make the protein required.
The Pfizer and Moderna vaccines contain one of these photocopies (mRNA) from the virus, which is designed to enter your cells, (not the nucleus), and tell your protein machinery how to make one part of the virus and display it on the outside of the cell. Your body then recognises this as an intruder and makes antibodies to it. If you then get infected by the real Covid-19 virus, your body is already prepared to fight it, helping eliminate it much more quickly.
So, although the mRNA enters your cells, it not only gets nowhere near your DNA, but it is also not possible for mRNA to alter DNA, any more than a photocopy of a recipe can alter the recipe book itself.
31. The Covid-19 vaccine will give me Covid-19.
None of the Covid-19 vaccines contain the virus itself and so cannot infect you with Covid-19. They all use different methods of introducing just the spike protein of the virus to your immune system. The spike protein alone cannot reform into the complete virus. Back to menu…
32. People are suffering all sorts of horrendous side effects after having the vaccine, which the government is trying to keep hidden.
Both parts of that statement are untrue.
There are multiple different surveillance operations set up to pick up, monitor and track any side effects. These form the most intense and comprehensive vaccine safety programme in history. In the UK, the Medicines and Healthcare products Regulatory Authority (MHRA) has a ‘Yellow Card’ scheme, where any member of the public can report suspected side effects. The COVID-19 Vaccine Safety Technical (VaST) Subgroup in the US meets weekly to review all available data and has reported on larger numbers than the UK. They monitor self-reported events, community surveillance programs, and doctor-reported events. Initially they are relying on VAERS (Vaccine Adverse Event Reporting System), the site where you can register any adverse effects following the vaccine. It is important to note that both the “Yellow Card” and the VAERS are sites where anyone can register an event, with no proof they’ve even had the vaccine, let alone evidence that the effect was caused by the vaccine. This leaves it open to abuse from people wishing to spread mistrust of the vaccines.
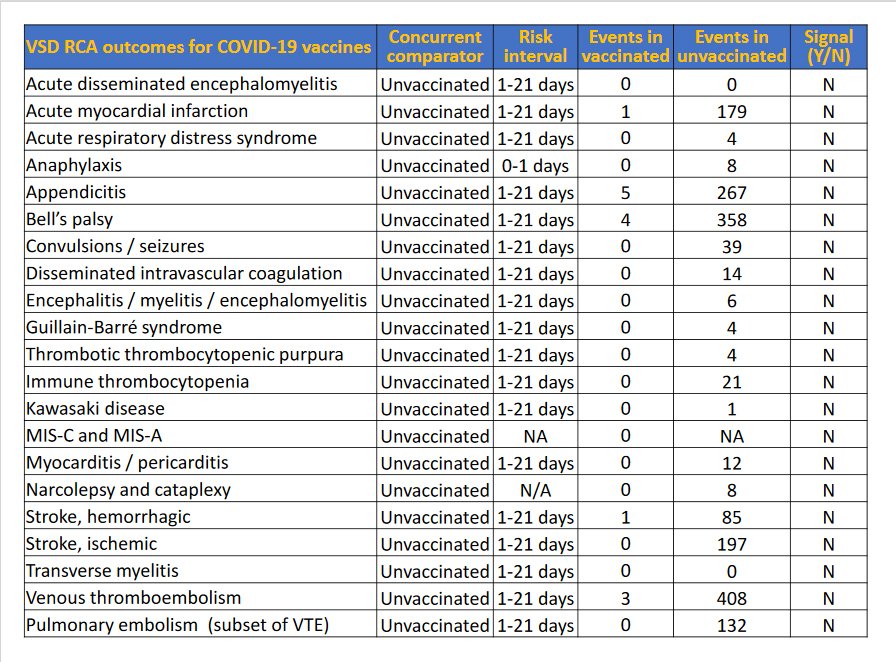
Bearing all that in mind, there had been 979 reported Serious Adverse Events (AE), and 8,117 reported non-serious Adverse Events by the middle of January in the US, following 21 million doses of the vaccine having been administered. Below are tables taken from Advisory Committee on Immunization Practices (ACIP) January 27, 2021 showing the most commonly reported non-serious AE and the Serious AE reported. The second table compares the number of reports of each event with how many times you would expect to see that event happening by pure chance in an unvaccinated population of the same size.
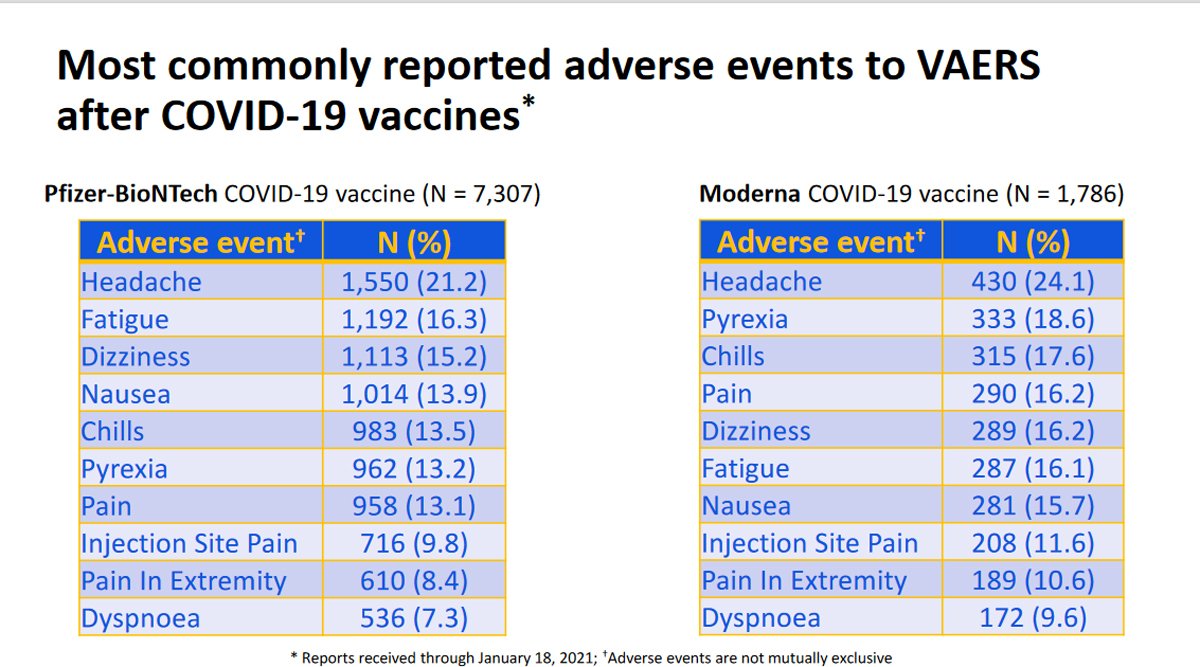
So people are experiencing some mild side effects, which are to be expected following any vaccination, including a sore arm, mild headache, dizziness etc. But there have been no serious side effects linked to the Covid-19 vaccine so far, despite millions of people having been vaccinated, with the exception of some cases of a severe allergic reaction (anaphylaxis) following vaccination. This was seen in some of the early vaccinated population, was very quickly raised as a potential issue, and is being monitored very closely. It is thought to occur in between 2.8 and 5.0 per million doses, so very rare. But in response to the issue, it has been recommended that patients should be checked for risk prior to vaccination and monitored for symptoms post-vaccination.
‘Yellow Card’ data in the UK is also being analysed, and has shown similar patterns to the data seen in the US. No deaths have been linked to the vaccine so far, and no serious side effects have been observed at any greater frequency than in a non-vaccinated population. The idea that anyone is trying to hide the side effects is simply not true. With clinical trial patients continuing to be followed up, multiple programs set up to allow both self-reporting and medical professional reporting, not to mention the world’s press waiting to jump on any story surrounding the vaccines, we can be very reassured that if there were any problems, they would be picked up fast. The anaphylaxis response shows how that works. Back to menu…
33. The COVID-19 vaccine contains microchips.
No, they really don’t! There is absolutely no evidence that the vaccines contain microchips. Nor any evidence that injected microchips would be able to control you. This is all science-fiction-type thinking.
The idea that scientists, governments, doctors, and the regulatory bodies approving the vaccines, would all collaborate across the world to inject people with microchips, and not a single person would go public with that information, is ludicrous. All the big tech companies are already able to track pretty much everywhere we go using our phones and everything we buy or look at online, so they really don’t need injectable microchips to achieve that! Back to menu…
34. The Covid-19 vaccine contains cells from aborted foetuses and monkey DNA.
This is a myth seemingly based on a misunderstanding about the Astra Zeneca vaccine and how it is created. The vaccine is made from an adenovirus (a type of virus that causes colds in chimpanzees) that is genetically altered. Firstly, this is to make sure it cannot cause infection, and secondly to add the genetic code for the Covid-19 spike protein. When this is injected into the body, our immune system gets primed to defend against the spike protein, giving us protection if we get infected by Covid-19.
Adenoviruses need to be grown in cells and scientists discovered some cells, called HEK293 cells, that were particularly good at growing adenoviruses, forming mini adenovirus factories. The first HEK293 cells came from a foetus aborted for personal reasons in 1973. The cells being used today grew from these original cells – but are not the exact cells from the foetus.
As the adenoviruses replicate inside the cells, they burst out, destroying the cells in the process. The adenovirus is then purified, removing all cell fragments, to create the vaccine. So although the vaccine is manufactured in these cells, there are no foetal cells in the vaccine itself. And although the idea of foetal cells sounds upsetting, it’s important to realise that no pregnancies have been terminated to produce them.
As for the ‘monkey’ DNA, again this seems to be a misunderstanding. The vaccine contains DNA from a virus known to infect chimpanzees. It does not contain chimpanzee (or monkey) DNA.

In conclusion, there is, unfortunately, a huge amount of misinformation out there; some based on misunderstandings, but sadly some being spread in a deliberate attempt to persuade people that Covid-19 is not that serious, and to put people off being vaccinated. This is extremely dangerous during a global pandemic, which is why it is so important to get your facts from reliable sources.



